


Most downloaded
- Page Path
-
- HOME
- BROWSE ARTICLES
- Most downloaded
"Most downloaded" articles are updated on a quarterly basis. The following are the most frequently downloaded articles from Annals of Coloproctology in the preceding months.
- Anorectal benign disease
- Immediate sphincter repair following fistulotomy for anal fistula: does it impact the healing rate and septic complications? (97 times)
- Maher A. Abbas, Anna T. Tsay, Mohammad Abbass
- Ann Coloproctol. 2024;40(3):217-224. Published online June 28, 2024
-
 Full text
Full text  PubReader
PubReader  ePub
ePub  Citation
Citation  PDF
PDF
- Colorectal cancer
- Postoperative outcomes after prehabilitation for colorectal cancer patients undergoing surgery: a systematic review and meta-analysis of randomized and nonrandomized studies (104 times)
- Ian Jun Yan Wee, Isaac Seow-En, Aik Yong Chok, Eileen Sim, Chee Hoe Koo, Wenjie Lin, Chang Meihuan, Emile Kwong-Wei Tan
- Ann Coloproctol. 2024;40(3):191-199. Published online May 16, 2024
-
Full text PubReader ePub Citation PDF
- ERAS
- Clinical impact of a multimodal pain management protocol for loop ileostomy reversal (79 times)
- Jeong Sub Kim, Chul Seung Lee, Jung Hoon Bae, Seung Rim Han, Do Sang Lee, In Kyu Lee, Yoon Suk Lee, In Kyeong Kim
- Ann Coloproctol. 2024;40(3):210-216. Published online June 19, 2024
-
Full text PubReader ePub Citation PDF

- Anorectal benign disease
- Long-term outcomes of sacral neuromodulation for low anterior resection syndrome after rectal cancer surgery (86 times)
- Mario J. de Miguel Valencia, Gabriel Marin, Ana Acevedo, Ana Hernando, Alfonso Álvarez, Fabiola Oteiza, Mario J. de Miguel Velasco
- Ann Coloproctol. 2024;40(3):234-244. Published online June 25, 2024
-
Full text PubReader ePub Citation PDF
- Minimally invasive surgery
- Preoperative localization of potentially invisible colonic lesions on the laparoscopic operation field: using autologous blood tattooing (72 times)
- Ji Yeon Mun, Hyunjoon An, Ri Na Yoo, Hyeon-Min Cho, Bong-Hyeon Kye
- Ann Coloproctol. 2024;40(3):225-233. Published online June 19, 2024
-
Full text PubReader ePub Citation PDF

- Video clip
- Cranial-first approach for laparoscopic extended right hemicolectomy (71 times)
- Kyong-Min Kang, Heung-Kwon Oh, Hong-Min Ahn, Tae-Gyun Lee, Hye-Rim Shin, Mi-Jeong Choi, Duck-Woo Kim, Sung-Bum Kang
- Ann Coloproctol. 2024;40(3):282-284. Published online June 19, 2024
-
Full text PubReader ePub Citation PDF
 Supplementary Material
Supplementary Material
- Colorectal cancer
- Partial mesorectal excision can be a primary option for middle rectal cancer: a propensity score–matched retrospective analysis (110 times)
- Ee Jin Kim, Chan Wook Kim, Jong Lyul Lee, Yong Sik Yoon, In Ja Park, Seok-Byung Lim, Chang Sik Yu, Jin Cheon Kim
- Ann Coloproctol. 2024;40(3):253-267. Published online March 31, 2023
-
Full text PubReader ePub Citation PDF
- Technical tips
- Transvaginal removal of rectal stromal tumor with Martius flap interposition: a feasible option for a large tumor at the anterior wall of the rectum (72 times)
- Weerapat Suwanthanma, Ploybutsara Kittiwetsakun, Samart Phuwapraisirisan, Pitichote Hiranyatheb
- Ann Coloproctol. 2024;40(3):276-281. Published online June 26, 2024
-
Full text PubReader ePub Citation PDF
- ERAS
- Venous thromboembolism among Asian populations with localized colorectal cancer undergoing curative resection: is pharmacological thromboprophylaxis required? A systematic review and meta-analysis (87 times)
- Shih Jia Janice Tan, Emile Kwong-Wei Tan, Yvonne Ying Ru Ng, Rehena Sultana, John Carson Allen, Isaac Seow-En, Ronnie Mathew, Aik Yong Chok
- Ann Coloproctol. 2024;40(3):200-209. Published online May 16, 2024
-
Full text PubReader ePub Citation PDF
- Colorectal cancer
- Obstructing colorectal cancer: a population-based review of colonic stenting in Queensland, Australia (68 times)
- Cian Keogh, Julie Moore, Danica Cossio, Nick Smith, David A. Clark
- Ann Coloproctol. 2024;40(3):268-275. Published online June 25, 2024
-
Full text PubReader ePub Citation PDF
- Colon cancer: the 2023 Korean clinical practice guidelines for diagnosis and treatment (179 times)
- Hyo Seon Ryu, Hyun Jung Kim, Woong Bae Ji, Byung Chang Kim, Ji Hun Kim, Sung Kyung Moon, Sung Il Kang, Han Deok Kwak, Eun Sun Kim, Chang Hyun Kim, Tae Hyung Kim, Gyoung Tae Noh, Byung-Soo Park, Hyeung-Min Park, Jeong Mo Bae, Jung Hoon Bae, Ni Eun Seo, Chang Hoon Song, Mi Sun Ahn, Jae Seon Eo, Young Chul Yoon, Joon-Kee Yoon, Kyung Ha Lee, Kyung Hee Lee, Kil-Yong Lee, Myung Su Lee, Sung Hak Lee, Jong Min Lee, Ji Eun Lee, Han Hee Lee, Myong Hoon Ihn, Je-Ho Jang, Sun Kyung Jeon, Kum Ju Chae, Jin-Ho Choi, Dae Hee Pyo, Gi Won Ha, Kyung Su Han, Young Ki Hong, Chang Won Hong, Jung-Myun Kwak, Korean Colon Cancer Multidisciplinary Committee
- Ann Coloproctol. 2024;40(2):89-113. Published online April 30, 2024
-
Full text PubReader ePub Citation PDF Supplementary Material
- The management of complex fistula in ano by transanal opening of the intersphincteric space (TROPIS): short-term results (155 times)
- Shrivats Mishra, Dileep S. Thakur, Uday Somashekar, Amrendra Verma, Dhananjay Sharma
- Received November 22, 2022 Accepted January 1, 2023
-
DOI: https://doi.org/10.3393/ac.2022.01018.0145 [Epub ahead of print]
-
Full text PubReader ePub Citation PDF
- Annual long-term functional outcomes after transanal repair for symptomatic rectocele (44 times)
- Akira Tsunoda, Hiroshi Kusanagi
- Received April 22, 2022 Accepted July 7, 2022
-
DOI: https://doi.org/10.3393/ac.2022.00283.0040 [Epub ahead of print]
-
Full text PubReader ePub Citation PDF
- Anorectal benign disease
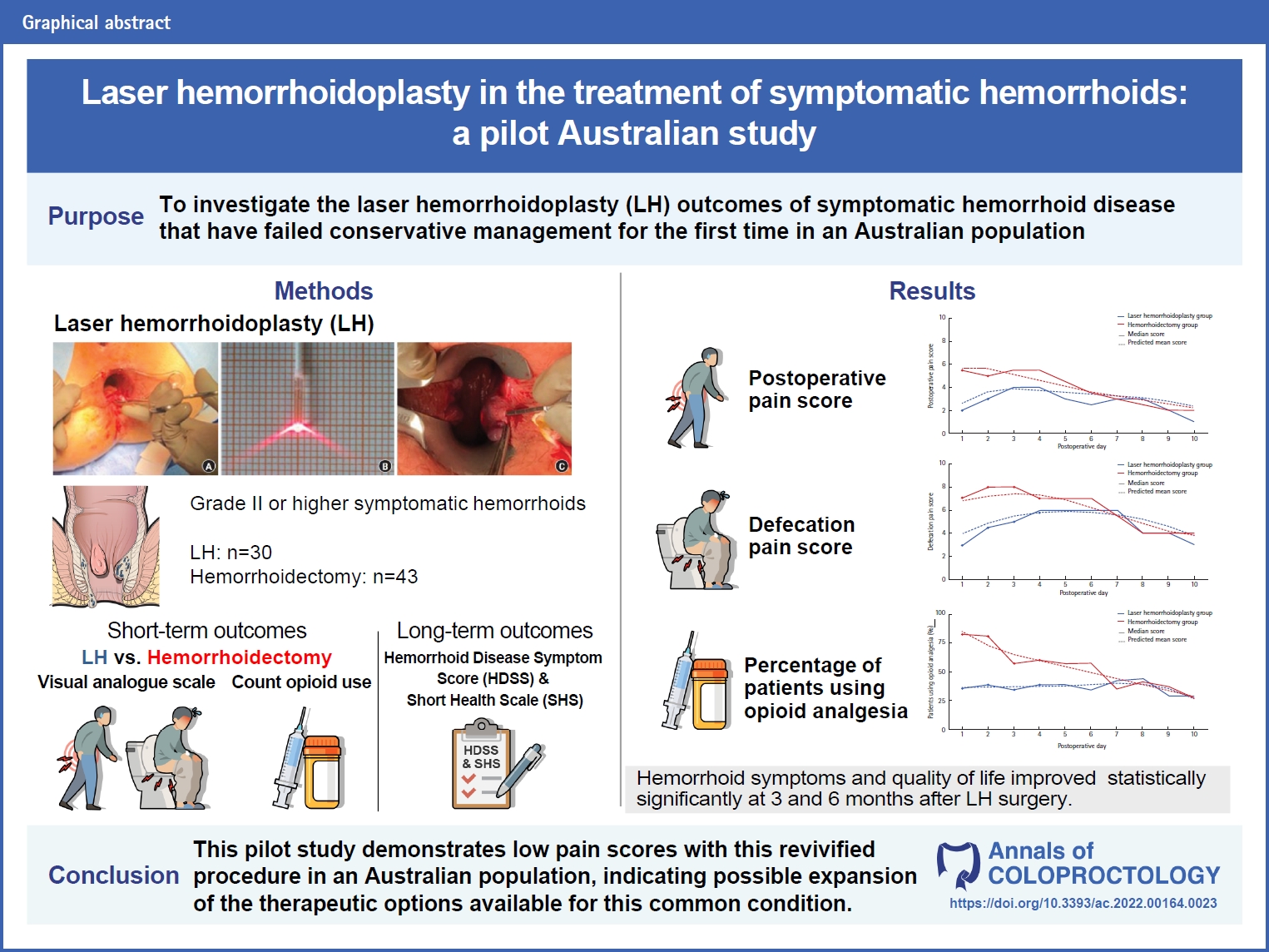
- Laser hemorrhoidoplasty in the treatment of symptomatic hemorrhoids: a pilot Australian study (430 times)
- Anshini Jain, Chen Lew, Gamze Aksakal, Richard Hiscock, Naseem Mirbagheri
- Ann Coloproctol. 2024;40(1):52-61. Published online May 19, 2022
-
Full text PubReader ePub Citation PDF
- Benign bowel disease
- Implications of bacteriological study in complicated and uncomplicated acute appendicitis (80 times)
- Sorin Cimpean, Alberto Gonzalez Barranquero, Ion Surdeanu, Benjamin Cadiere, Guy-Bernard Cadiere
- Received February 28, 2022 Accepted July 7, 2022
-
DOI: https://doi.org/10.3393/ac.2022.00157.0022 [Epub ahead of print]
-
Full text PubReader ePub Citation PDF
- Laser hemorrhoidoplasty versus conventional hemorrhoidectomy for grade II/III hemorrhoids: a systematic review and meta-analysis (279 times)
- Ian Jun Yan Wee, Chee Hoe Koo, Isaac Seow-En, Yvonne Ying Ru Ng, Wenjie Lin, Emile John Kwong-Wei Tan
- Ann Coloproctol. 2023;39(1):3-10. Published online January 3, 2023
-
Full text PubReader ePub Citation PDF Supplementary Material








- ARTICLE CATEGORY
- Editorial Office
-
Room 1519, Suseo Hyundai Venture-vill, 10 Bamgogae-ro 1-gil, Gangnam-gu, Seoul 06349, Korea
Tel: +82-2-2040-7737 Fax: +82-2-2040-7735 E-mail: editor@coloproctol.org
Copyright © 2024 by Korean Society of Coloproctology.

