INTRODUCTION
Complicated intra-abdominal infections represent a widespread problem, encountered worldwide, with appendicitis alone affecting 300,000 patients/year and consuming >1 million hospital days in the United States [1]. The lifetime risk is estimated to be 8.6% in men and 6.7% in women [2].
This pathology is well-known and the etiology is related usually with an obstruction of the appendix lumen. Other pathologies that can produce an inflammation of the appendix are tumors (carcinoid tumors and adenocarcinoma), intestinal parasites, and hypertrophied lymphatic tissue [3].
Acute appendicitis is treated by appendectomy and is usually followed by additional antibiotic treatment. In case of necrosis or perforation of the appendix with secondary peritonitis, the antibiotherapy is important for the treatment and prevention of the postoperative infectious complications. Antibiotic use can be considered as an adjunct to surgical intervention, and their appropriate use remains a critical aspect [4]. The bacteriological sample in case of presence of intra-abdominal free fluid is necessary to adapt the antibiotherapy and to prevent the development of resistance. In case of simple appendicitis, restriction of antibiotic treatment can be considered.
The bacterial flora in the appendix consists of a mixture of aerobes and anaerobes bacteria. In the literature, Escherichia coli and Bacteroides fragilis are most commonly associated with appendicitis, and the first-line empiric antibiotic therapy is typically selected to target these bacteria [5]. Nevertheless, acute appendicitis is habitually a polymicrobial infection, with up to 14 different bacteria reported [6].
The aim of the study is to evaluate the differences between uncomplicated acute appendicitis (UAA) and complicated acute appendicitis (CAA) in terms of bacterial culture results and antibiotic resistance. The secondary outcome was to evaluate the predictors for complicated appendicitis. The study also evaluates the clinical implication of the bacterial culture results of UAA and CAA in term of antibiotic resistance, and the risk factor of CAA.
METHODS
Ethics statement
The study was approved by the Ethics Committee of Saint Pierre University Hospital. The verbal/oral informed consent was obtained in consultation, by telephone or by email from the patients or the legal representative.
Study design
We performed a single-center, retrospective observational study of all consecutive patients who presented with appendicular peritonitis and underwent emergent surgery in Saint Pierre University Hospital (Brussels, Belgium), between January 2013 and December 2020.
The inclusion criteria for the 268 patients analyzed were the patients over 15 years old, who underwent an appendectomy in an emergent surgery, with the presence of peritonitis of appendicular origin, and enough quantity of intra-abdominal free fluid to allow the bacteriological sample.
The exclusion criteria were peritonitis of a distinct origin, conservative or percutaneous treatment of appendicular abscess, the absence of free fluid, the absence of bacteriological sample, or the absence of bacteriological analysis.
Intervention
All patients with the diagnosis of acute appendicitis who underwent emergent surgery received amoxicillin/clavulanic acid as preoperative antibiotic treatment, in the absence of previous allergies. The periappendicular intra-abdominal free fluid visualized during the surgery was collected in sterile conditions and was sent for bacteriological analysis. Postoperative antibiotics were prescribed depending on the clinical condition of the patient and the state of the surgical field during the intervention. Tailored antibiotic therapy was adjusted according to the results of the antibiotic sensitivity testing, usually available 48 hours after the surgery, especially in cases of antibiotic resistance. A systematic blood test was performed on the second postoperative day to follow the dynamics of the inflammatory syndrome. The patient was discharged in the absence of relevant postoperative complications.
Variables
Baseline characteristics collected were age, sex, nationality, Charlson Comorbidity Index (CCI; which predicts the 10-year mortality for a patient according to their comorbid conditions), and personal history of abdominal surgery or other surgeries. At admission, the physical examination signs analyzed were heart rate, systolic blood pressure, and body temperature; and the C-reactive protein and the white blood cell (WBC) count from the blood tests. The type of surgical intervention, the open or laparoscopic approach, and the need for drainage were the intraoperative variables analyzed.
A positive bacteriological analysis was thoroughly evaluated to identify the specific bacteria and their resistance to the antibiotic. We also evaluated the antibiotic treatment prescribed, in the first-, second-, and third-line.
Postoperative variables were the hospital stay, blood tests at 48 hours after surgery, overall morbidity and its severity according to the Clavien Dindo classification [9], and the need for reintervention. Specific complications analyzed were postoperative ileus, acute kidney injury, bacteremia, surgical site infection, and cecal perforation.
Statistical analysis
Categorical variables were described with numbers and percentages. Quantitative variables were described with mean and standard deviation if they followed a normal distribution and with median and interquartile range (IQR) if they followed a non-normal distribution. The Shapiro-Wilk test was used as a normality test.
To evaluate the null hypothesis, the chi-square test was used for categorical variables, the Student t-test was used for normal quantitative variables and the Mann-Whitney U-test was used for non-normal quantitative variables.
All variables were tested in univariate logistic regression to explore the factors linked with complicated appendicitis, except for specific bacterial isolation with <10 positive cultures. Statistically significant variables in univariate analysis were then included in a multivariable logistic regression model, erasing nonsignificant outcomes until all variables were adjusted to each other in the final model. A P-value of <0.05 in a 2-tailed statistical analysis was considered statistically significant. Statistical analysis was performed with IBM SPSS ver. 23.0 (IBM Corp).
RESULTS
A total of 834 patients were operated for acute appendicitis during the period of the study. We included 268 patients (161 with UAA and 107 with CAA) after excluding 566 patients according to the exclusion criteria, mainly due to the absence of sufficient free fluid for bacteriological analysis.
The demographic analysis (Table 1) revealed that patients in the CAA group were older (38.5 years [IQR, 27.0ŌĆō52.0 years] vs. 33.5 years [IQR, 25.3ŌĆō41.0 years]), and there was a higher proportion of male patients in this group (71.0% vs. 56.5%). These differences were statistically significant. There were no statistically significant differences in the nationality between groups.
Patients in the UAA group presented more personal history of abdominal surgeries (26 [16.1%] vs. 14 [13.1%]) and more personal history of other surgeries (18 [11.2%] vs. 10 [9.3%]), with no statistical significance.
Although the median CCI was 0 for both groups, the IQR was discretely higher in the CAA group (0ŌĆō1 vs. 0ŌĆō0), thus there was a statistically significant difference (P=0.017).
Initial evaluation of the patients
The general condition of the patients was evaluated at the hospital admission and the patient parameters were evaluated. The analysis of the clinical parameters found statistically significant differences, with an increased heart rate in the CAA group (95 beats per minute [bpm] [IQR, 81.0ŌĆō108.0 bpm] vs. 87 bpm [IQR, 76.0ŌĆō100.5 bpm]), the prevalence of tachycardia in the CAA group (46 [43.0%] vs. 48 [29.8%]) and an increased body temperature in the patients with CAA (18 [16.8%] vs. 19 [11.8%]).
The inflammatory syndrome was more important in the CAA group and reflected by the levels of C-reactive protein (97.5 g/dL [IQR, 29.6ŌĆō188.3 g/dL] vs. 29.2 g/dL [IQR, 6.5ŌĆō101.0 g/dL]) and WBC count (15,720/mm3 [IQR, 12,040ŌĆō18,500/mm3] vs. 13,460/mm3 [IQR, 8,216ŌĆō16,170/mm3]). These differences were statistically significant.
Surgical treatment
A higher proportion of surgeries were performed by laparoscopy in the UAA group (156 [96.9%] vs. 91 [85.0%]). Patients with UAA received more appendectomies (158 [98.1%] vs. 99 [92.5%]) and ileocecal resections (2 [1.2%] vs. 1 [0.9%]), while the CAA group presented more cecectomies (7 [6.5%] vs. 1 [0.6%]).
The CAA presented more contamination of the peritoneal cavity, and the drainage was considered useful by the surgeon in most patients. The drain was placed in case of presence of cloudy or purulent peritoneal liquid. The abdominal drainage was more frequently used in the CAA group (84 [78.5%] vs. 83 [51.6%]) and placed in periappendicular (59 [55.1%] vs. 42 [26.1%]) or pelvic position (57 [53.3%] vs. 63 [39.1%], P=0.025).
Bacterial culture
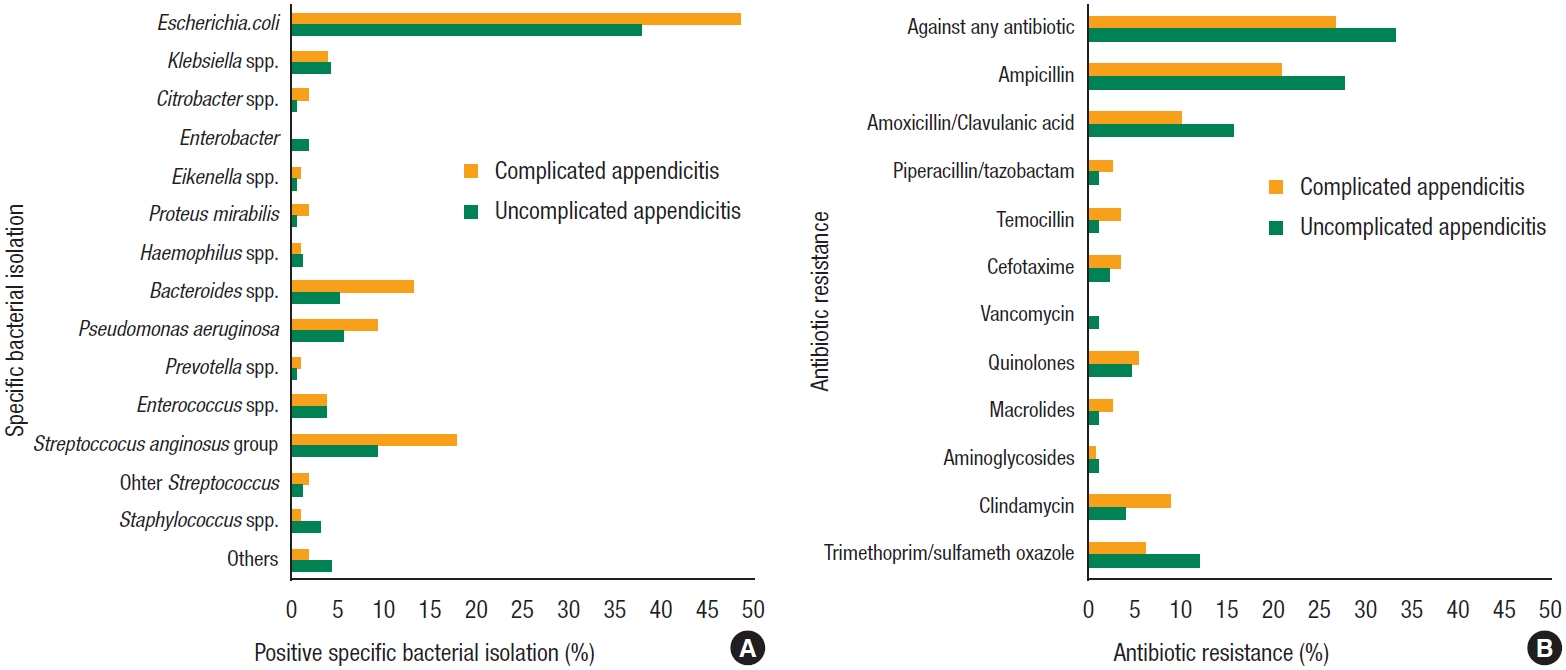
The positive microbiological culture rate was, as expected, significantly higher in the CAA group (73 [68.2%] vs. 86 [53.4%]) (Table 2). Statistically significant differences were observed in the bacterial isolation, with an increased proportion of gram-negative bacteria in CAA cultures (65 [60.7%] vs. 76 [47.2%]), while there were no differences in the proportion of gram-positive or anaerobic bacteria between groups.
The most frequently isolated bacteria in UAA cultures were E. coli (61, 37.9%), bacteria from the Streptococcus anginosus group (15, 9.3%), Pseudomonas aeruginosa (9, 5.6%), Bacteroides spp. (8, 5.0%), and Klebsiella spp. (7, 4.3%). In the CAA group the most frequently isolated bacteria were E. coli (52, 48.6%), bacteria from the S. anginosus group (19, 7.8%), Bacteroides spp. (14, 13.1%), P. aeruginosa (10, 9.3%), and Klebsiella spp. (4, 3.7%). Other isolated bacteria were Citrobacter spp., Enterobacter, Eikenella spp., Proteus mirabilis, Haemophilus spp., Prevotella spp., Enterococcus spp., other Streptococcus, and Staphylococcus spp. (Fig. 1).
Antibiotic treatment
No significant differences were observed between the 2 groups in terms of antibiotic resistance, with an overall rate of antibiotic resistance of 34.2% (55 of 161) in the UAA group and 27.1% (29 of 107) in the CAA group. The most common resistances observed were against ampicillin (46 [28.6%] and 23 [21.5%]) and amoxicillin/clavulanic acid (26 [16.1%] and 11 [10.3%]) in the UAA and CAA groups, respectively. Other relevant resistances found were against trimethoprim/sulfamethoxazole (20, 12.4%) and clindamycin (10, 9.3%) in the UAA and CAA groups, respectively. There was a low resistance rate against quinolones in the UAA group (8, 5.0%) and CAA group (6, 5.6%) (Fig. 1).
More patients in the UAA group received monotherapy as the first-line of antibiotic treatment (154 [95.7%] vs. 100 [93.5%]) and none received combined therapy (0 [0%] vs. 5 [4.7%]). Most patients received amoxicillin/clavulanic acid as the first-line of treatment (94.4% in the UAA group and 89.7% in the CAA group). There were resistances to the first-line of antibiotic treatment in 27 patients (16.8%) from the UAA group versus 10 patients (9.3%) from the CAA group, without statistically significant differences.
For the second-line of antibiotics, most patients received piperacillin/tazobactam (5.0% in the UAA group and 4.7% in the CAA group). There was only 1 resistance (0.9%) to this line of treatment in the CAA group, without statistically significant differences.
The third-line of treatment was not necessary mostly for patients with UAA (159 [98.8%] vs. 103 [96.3%]). Levofloxacin-ornidazole and piperacillin/tazobactam were the most commonly used antibiotics in both groups. The median antibiotic duration was statistically significantly higher in the CAA group (5.5 days [IQR, 3ŌĆō7 days] vs. 5 days [IQR, 2ŌĆō7 days]).
Postoperative outcomes
In term of postoperative outcomes, the morbidity was significantly higher for patients with CAA (21 [19.6%] vs. 11 [6.8%]). Thirty-day complications according to Clavien-Dindo classification revealed a significant difference for the CAA group, with a higher proportion of grade I, II, and III complications. There was a higher proportion of surgical site infections in the CAA group (14 [13.1%] vs. 8 [5.0%]) as a specific complication.
The C-reactive protein level at 48-hour postoperative blood test was higher in the CAA group (202.4 mg/dL [IQR, 96.6ŌĆō316.0 mg/dL] vs. 111.9 mg/dL [IQR, 28.9ŌĆō215.7 mg/dL]), with a similar WBC count between groups.
The hospital stay was significantly longer in the CAA group (5 days [IQR, 3ŌĆō6 days]) than in the UAA group (3 days [IQR, 2ŌĆō5 days]) (Table 3).
Analysis of factors linked with complicated appendicitis
All variables were evaluated as factors linked with complicated appendicitis. Variables with statistical significance in univariate analysis to predict complicated appendicitis and the results from the most common specific bacterial isolation are shown in Table 4. Once adjusted in multivariate analysis the risk factors related to complicated appendicitis were the CCI, the WBC count at admission, the need for an open procedure, and the need for surgical drainage. All variables that could be considered risk factors were tested in univariate logistic regression to explore if they were linked with complicated appendicitis, except for specific bacterial isolation with <10 positive cultures (Table 4). Neither the culture results, the group of bacterial isolation, or the specific isolated bacteria could predict complicated appendicitis.
DISCUSSION
Acute appendicitis is the most common cause of acute peritonitis, with 7% of cases of secondary diffuse peritonitis. In case of complicated appendicitis, perforated appendicitis with peritonitis, the morbidity is increased. Diffuse peritonitis represents the most severe grade of CAA, and it is still considered an important cause of morbidity (10%) and mortality (1%ŌĆō2.5%) [10].
In some studies, gram-negative bacteria are more common in acute appendicitis compared to gram-positive [11, 12]. Garc├Ła-Mar├Łn et al. [13] found that the culture-positive rate was higher in CAA than in UAA, identifying a higher frequency of gram-positive cocci and anaerobic bacteria with different isolates and susceptibilities. Parthiban and Harish [14] in a microbiology study of the appendicectomy specimen showed that anaerobes acted as the commonest organism involved in appendicitis and postoperative wound infection. Moreover, the presence of anaerobes caused a higher incidence of complicated appendicitis. Lafi et al. [15] found that the most common bacteria found in a bacteriological study of acute appendicitis were E. coli, B. fragilis, and Staphylococcus aureus. For Chen et al. [3], the most commonly involved bacteria were E. coli, followed by Klebsiella pneumoniae, Streptococcus spp., Enterococcus spp., and P. aeruginosa. The presence of P. aeruginosa was associated with wound infection, despite antibiotic prophylaxis, highlighting that special consideration for the clinical and biological evolution of these patients was necessary when this pathogen was found [16]. In our study, the most frequently identified bacteria were gram-negative, especially in the setting of CAA, without statistically significant differences between groups in the presence of gram-positive or anaerobes. However, there was no association between the group of bacterial isolation or the specific isolated bacteria and the presentation of a CAA.
In recent years, multiple studies revealed that in case of UAA, the antibiotics only can be a reliable treatment. APPAC (Appendicitis Acuta) randomized clinical trial found that in case of UAA, the antibiotic treatment for did not require appendectomy during the 1-year follow-up period, and those who required appendectomy did not experience significant complications [17, 18]. In case of simple appendicitis, the inferiority of nonoperative therapy vs. appendectomy could equally be related to the type of antibiotic used. Current evidence show that resistance of E. coli to amoxicillin plus clavulanic acid is increasing [19].
There is a real concern about the antibiotic resistance of the bacteria. The resistant and virulent microorganisms might be a result of antibiotic exposure or the application of invasive and prolonged medical and surgical treatment [20]. The presence of multidrug-resistant bacteria can contribute to additional morbidity [21]. In a study from 2010, 25% of children with gangrenous or ruptured appendicitis were insensitive to the antimicrobial regime used [22]. E. coli and mixed anaerobes are the predominant organisms identified in secondary peritonitis from appendicitis in children. In case of an inadequate empirical antibiotic and amoxicillin/clavulanate resistance of the bacteria, postoperative infectious complications might increase [23].
The initial empirical therapy should target all of the microorganisms likely to be involved, on the basis of the suspected risk factors [24]. Empiric antibiotic treatment is effective in most patients, early (blood or intra-abdominal) culturing is very useful to guide antibiotic modification in abdominal infection [25]. If the postoperative evolution of the patient is not optimal, the results of the bacterial culture are critical, especially in the actual tendency of increased occurrence of multidrug-resistant bacterial strains [26].
Andersen et al. [27] in a review of literature found that the antibiotic prophylaxis is effective in the prevention of postoperative complications in appendectomies patients, whether the administration is given preoperatively, perioperatively, or postoperatively. Kimbrell et al. [28] in a study on postoperative antibiotic administration in CAA suggest that the use of postoperative prophylactic antibiotics more than 24 hours in patients does not prevent the development of an abscess. Obinwa et al. [23] in a study on the microbiology of secondary bacterial peritonitis due to appendicitis found that inadequate initial empirical antibiotic and amoxicillin/clavulanate resistant E. coli may contribute to increased postoperative infectious complications. The study recommended a triple antibiotic combination of amoxicillin/clavulanate, gentamicin, and metronidazole as an empiric treatment in CAA.
The prospective multicenter study MUSTANG (Multicenter Study of the Treatment of Appendicitis in America: Acute, Perforated, and Gangrenous) on the duration of antibiotherapy found that there was no evidence of an association between the duration of 24 hours versus 96 hours for CAA and an increased rate of SSI [29]. A study from the Netherlands (2014) concluded that 3 days of antibiotics led to a similar rate of infectious complications of 5 days or more [30, 31]. In a meta-analysis by van den Boom et al. [32] revealed that there were no differences in the incidence of intra-abdominal abscess with Ōēż3 days versus >3 days of antibiotic treatment, but there was a reduction with >5 days of treatment. Xu et al. [33] in a retrospective analysis of 93 patients who underwent appendectomy found that the average stay of patients receiving fluoroquinolones was 2.6 days shorter than patients who received cephalosporins. In our study, the median duration of the antibiotic treatment was 5 days for UAA and 5.5 days for CAA. Therefore, the duration could have been optimized in the UAA but might have been optimal for the CAA group. In our institution, the antibiotics were discontinued, in concertation with the infectiology team accordingly to the type of bacteria culture and type of antibiotic.
In conclusion, the bacterial culture allows for not only evaluating the immediate impact of the antibiotics treatment and evaluating the resistance, but also evaluating the preoperative empirical treatments in order to reduce patientsŌĆÖ morbidity. CAA presented a higher rate of positive cultures with increased identification of gram-negative bacteria. E. coli, bacteria from the S. anginosus group, and Bacteroides spp. were the most commonly isolated bacteria, without relevant differences in terms of antibiotic resistance. The predictors for complicated appendicitis were preoperative or intraoperative variables, while the culture results, the group of bacterial isolation or the specific isolated bacteria did not predict complicated appendicitis.