INTRODUCTION
Anal fistula is a benign anorectal disorder characterized by an infected epithelized tract that develops between the perianal skin and the bowel. These develop in up to 40% of patients during the acute phase of perianal sepsis or may even be discovered 12 months after initial therapy [1].
A fistula in ano is termed complex when the tract crosses > 30% of the external sphincter, is recurrent, has multiple tracts, is associated with preexisting anal incontinence, has a history of local radiation, is secondary to diseases such as CrohnŌĆÖs disease, tuberculosis, HIV, and malignancy, or is anterior in females [2]. The management of complex fistula in ano remains a major surgical challenge and carries significant morbidity on account of damage to the anal sphincter.
It is now recognized that the intersphincteric space is more commonly involved in the development of complex fistula in ano than the deep postanal space, as described by Courtney [3]. This concept has led to new advances in the treatment of complex fistula in ano [4]. To treat sepsis in the deep intersphincteric space, there must be adequate drainage of the intersphincteric space, followed by curettage of the external tract to ensure proper wound healing. Conventional fistulotomy carries the risk of anal incontinence owing to sphincter division and recurrence due to incomplete excision. New modalities, such as the anal fistula plug (AFP), video-assisted anal fistula treatment (VAAFT), and over-thescope clips (OTSC), are associated with high recurrence rates in complex fistula in ano, as these modalities fail to adequately drain the area of sepsis in the intersphincteric space. Furthermore, they require special equipment, which adds to the cost of treatment.
Transanal opening of the intersphincteric space (TROPIS) is a novel method for the treatment of complex fistula in ano, in which the intersphincteric space is laid open through the transanal route. This properly addresses sepsis in the inter sphincteric space [5]. Unlike in other procedures, the intersphincteric space is not closed and is allowed to heal by secondary intention. TROPIS is a sphincter-sparing procedure. TROPIS can be done with conventional instruments, making it feasible in any surgical setting.
METHODS
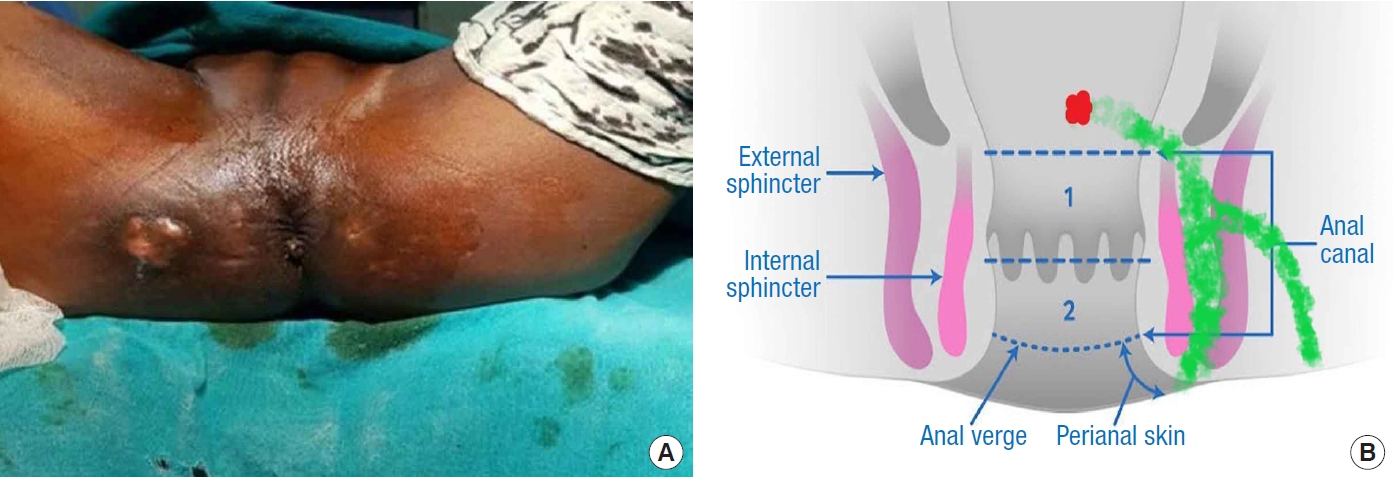
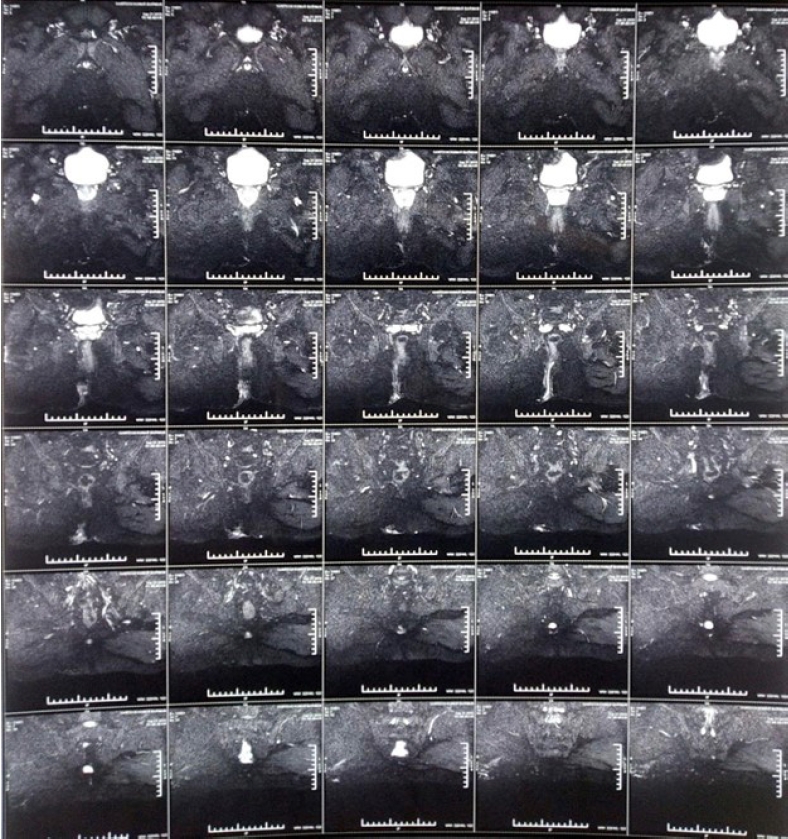
This prospective study was conducted at the Department of Surgery, NSCB Medical College from December 2018 to July 2020 after receiving approval from the Institutional Ethics Review Board. Informed consent was obtained from all patients. Thirtyfive consecutive patients with complex fistula in ano (i.e., with a fistula involving more than one-third of the sphincter complex (Fig. 1), as assessed on a baseline magnetic resonance fistulogram (Fig. 2) and clinical examination) or with a horseshoe fistula were included in the study. Patients with a low fistula (involving less than one-third of the sphincter complex) and those with associated conditions such as CrohnŌĆÖs disease, tuberculosis, malignancy, and radiation therapy were excluded.
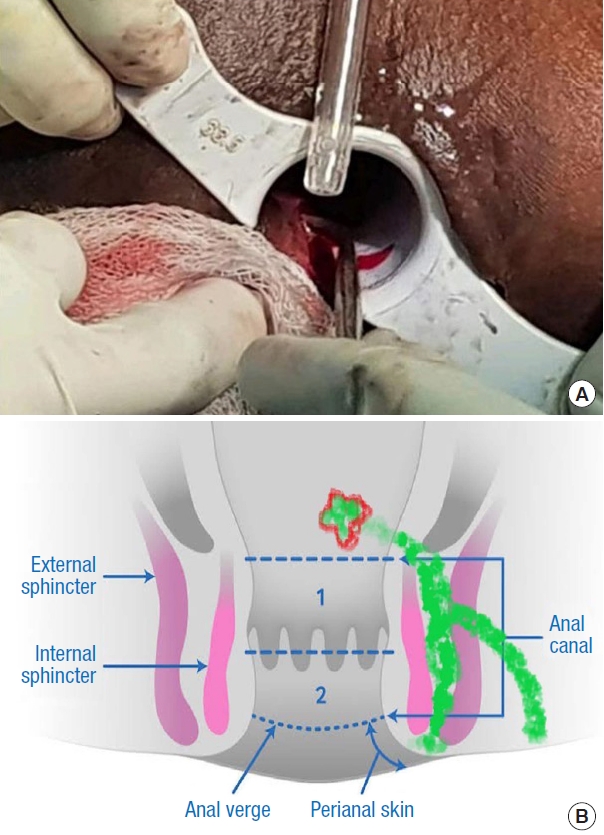
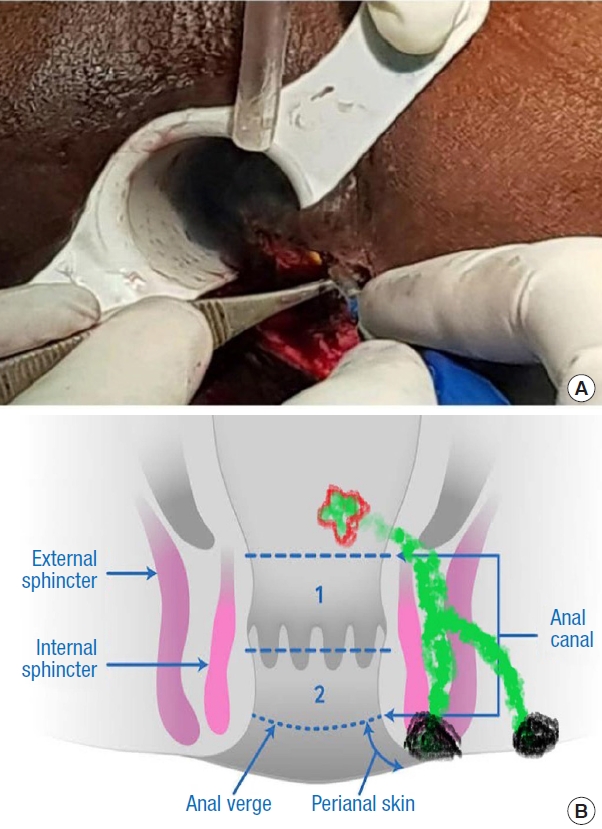
The baseline incontinence score was obtained using the St. MarkŌĆÖs incontinence score (SMIS) in all patients. Its parameters include the type and frequency of anal incontinence (gas, liquid, solid) and its impact on daily life, the need to wear a pad, the use of constipating medication, and the lack of ability to defer defecation for 15 minutes. The types of anal incontinence and its impact on daily life are each scored from 0 (never) to 4 (daily), the need to wear a pad and the need for medication are each scored 0 (no) or 2 (yes), and fecal urgency is assigned a score of 0 (no) or 4 (yes). This gives a range from 0 (complete continence) to 24 (complete incontinence) [6]. Bowel preparation was not done. Patients underwent surgery under saddle anesthesia, in lithotomy position, with an antibiotic (an injection of ceftriaxone with sulbactam, 1.5 g) given at the time of induction. An anoscope lubricated with 2% lignocaine jelly was inserted for visualization. The internal opening was located by the expression of hydrogen peroxide (H2O2) (Fig. 3) and diluted methylene blue was injected through the external opening. Under the visualization using the anoscope, the internal opening was identified. Artery forceps were inserted into the internal opening and the mucosa (Fig. 4) and the internal sphincter were incised over it, along the tract, in a curvilinear or oblique fashion. This laid open the length of the tract from the internal opening up to the external sphincter.
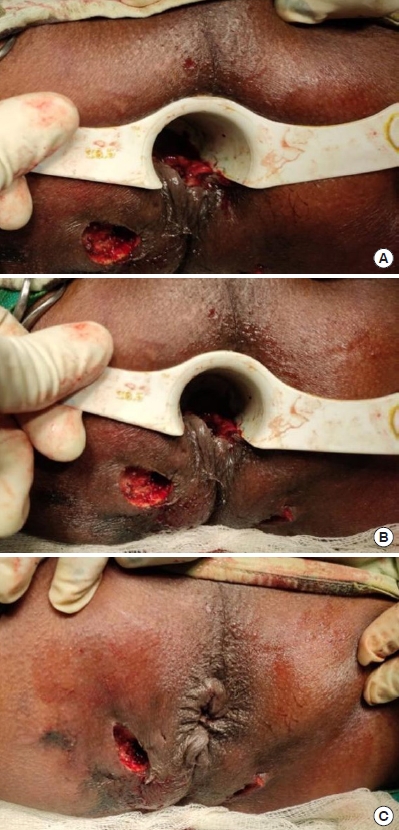
Next, the part of the tract between the external opening(s) and the external sphincter was curetted (Fig. 5). Thus, the external sphincter was preserved. Hemostasis was achieved. A wick was placed in the external opening to prevent its premature closure and to allow fluid pus to drain. A separate anal pack was placed. Curetted material from the tract was sent for a histopathological examination (Fig. 6).
Liquid feeding was resumed 2 hours after surgery. The anal pack was removed 6 hours after the procedure, and the anal region was observed for any active bleeding. A laxative (lactulose syrup, 2 teaspoons with half a glass of water) was given on the same day.
Patients were discharged the next day with advice for a sitz bath and topical metronidazole ointment, and they were advised to resume normal activities. Incontinence was reassessed using the SMIS on follow-up at weeks 2, 4, 8, and 12 postoperatively. Healing of the tract was also assessed at weeks 2, 4, 8, and 12. If pus was found over the external opening wound, it was considered a failure. A minor procedure of curettage under local anesthesia was done, and patients were followed up and reassessed for healing.
Statistical analysis was done using the chi-square test for categorical variables and the Student t-test for continuous variables. A P-value of < 0.05 was considered significant.
RESULTS
The demographic profile and fistula classification of the study population are shown in Table 1. The mean preoperative incontinence score was 0, and there was no significant change in the score postoperatively at 3 months, with a mean of 0.02. One patient developed incontinence to gas, with an SMIS score of 1 at the initial 2-week follow-up. This patient was further followed up and was continent by the end of 12 weeks.
DISCUSSION
The treatment of complex fistula in ano has evolved over the past few decades. Conventional methods such as fistulotomy and setons were associated with high postoperative morbidity, incontinence, and recurrence. The importance of the intersphincteric space being the focus of sepsis in complex fistulas was emphasized by Kurihara et al. [4] and Zhang et al. [7]. Newer modalities like AFP, VAAFT, OTSC clip, fibrin glue, and the fistula-tract laser closure (FiLaC) device fail to address this source of sepsis, resulting in failure of fistula closure.
TROPIS is a new procedure introduced for the treatment of complex fistula in ano. This initial study showed an overall healing rate of 90.4% without any deterioration of continence in a median 9 months of postoperative follow-up [5]. The same authors also demonstrated a success rate of 87.6%, with a maintained level of continence, in a larger cohort with long-term follow-up (median, 36 months) [8].
TROPIS involves drainage of the intersphincteric space, which is then left open, unlike in other new procedures for complex fistula in ano [9ŌĆō11]. Leaving the wound open in TROPIS allows healing of the wound by secondary intention and also aids in wound cleaning and curettage if pus drainage occurs during follow-up. Fistulotomy procedures also lay open the tract, which helps in drainage, but at the cost of postoperative incontinence in up to 24.2% to 62.8% of patients, depending upon the level of division of the external sphincter [12] as the external anal sphincter is not spared. In TROPIS, however, the external sphincter is spared, thus preserving continence. TROPIS fares favorably compared to other modalities in the management of complex fistula in ano (Table 2) [5, 8ŌĆō11, 13,ŌĆō17].
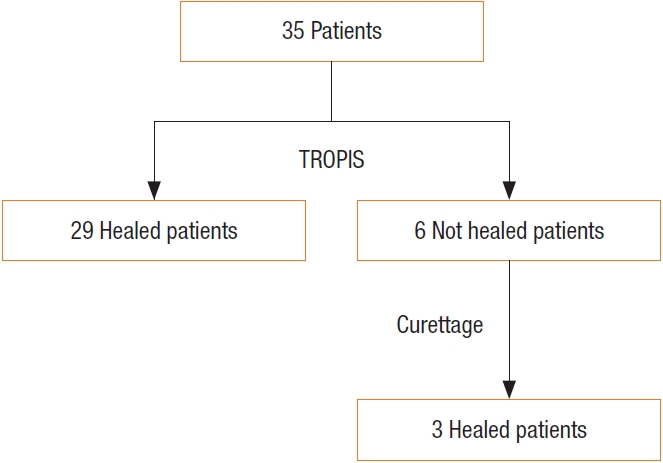
The fistula closure rate (91.4%) and the maintenance of continence in our study are similar to the outcomes of TROPIS reported in the literature [5]. During the follow-up period, we performed curettage of the external tract wound as an adjunct in patients whose wounds were unhealthy or had pus discharge. Curettage saved most patients from reoperation, 3 out of 6 patients (50%) whose fistula had not closed healed completely following curettage (Fig. 7). However, the need for repeated curettage has been described in some patients in previous studies. The limitations of our study were the relatively small sample size and the short follow-up period.
When considering treatment efficacy, a recent meta-analysis of 29 studies comparing the outcomes of different sphincter-sparing techniques for fistula in ano by Huang et al. [18] showed no significant difference among the techniques. However, TROPIS had the highest success rate. Furthermore, when an internal opening is not identified in complex fistulas, the TROPIS procedure applying the Garg protocol has helped to treat anal fistulas successfully [19, 20]. Moreover, there was very little risk of the postoperative deterioration of anal continence
Other advantages of TROPIS include the fact that it requires no special instruments, is easy to learn and to teach, and can be performed cost-effectively in small surgical setups in low- and middle-income countries, unlike other newer treatment modalities for complex fistula in ano.