INTRODUCTION
Colorectal cancer surgery using laparoscopy is one of the most widely used surgical techniques worldwide [1, 2]. After the introduction of laparoscopic surgery, it is gradually replacing open surgery [3, 4]. Conventional laparoscopic surgery has been further advanced, and studies have been conducted on surgical techniques that reduce the number of ports needed [5, 6]. Accordingly, a method using only 1 port was introduced. Single-incision laparoscopic surgery has the advantage of being limited to 1 surgical site with a small wound size [7, 8]. It is used for colorectal cancer surgery because it causes excellent in cosmetic terms without lagging behind conventional laparoscopy in oncologic outcomes. Now, new surgical methods that could replace the laparoscopic platform are developing. Improvements to laparoscopic surgery were needed due to the rigidity of the instrument, the narrow pelvic area available for the approach, and the hassle of camera adjustment. The safety and feasibility of using a robotic platform for surgery, one potential replacement for laparoscopy, were first tested in 2002 [9].
In 2018, a single-port robot (SPR) device was introduced by Intuitive Surgical Inc. Its feasibility and safety in urology and gynecology were recognized through intraperitoneal surgery [10–12]. However, few reports have been made about the safety of SPR for colorectal cancer surgery. Recently, results of SPR for left colectomy have been reported, and safety certification is beginning to be obtained [13].
Compared to single-incision laparoscopic surgery, when using the SPR device, the operator can operate more comfortably and easily. In addition, it has the advantage of being able to easily access the desired surgical field through a 3-dimensional view and a flexible camera. However, it takes a lot of effort and time to master the new technology. An easy way to check this objectively is to check the learning curve. The purpose of this study is to determine the number of surgeries required to reach a sufficient learning curve when a surgeon who has not previously experienced robotic surgery performed colon cancer surgery using a single-port da Vinci robotic device (Intuitive Surgical Inc). In addition, it is to analyze the occurrence of acute complications in surgery performed with the SPR device.
METHODS
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Samsung Medical Center (No. 2019-08-062). The informed consent of patients was waived due to the retrospective nature of the study, and written informed consent was obtained from patients for the publication of clinical images.
Patients
We reviewed 39 patients who underwent SPR colectomy surgery between April and October 2019. In this study, adults over 18 years of age who were diagnosed with colon cancer and underwent surgery were included. Prior to surgery, the patient’s preference for conventional operation and single-port operation was investigated. Among them, patients who wanted single-port operation were enrolled and proceeded. Cases not generally recommended for robotic surgery and excluded from this study are benign lesions, suspected adhesions due to a history of more than 2 previous abdominal operations, clinical or radiological evidence of intraabdominal metastases and subsequent adhesions expected, inflammatory bowel disease, anal canal cancer, and locally advanced cancers not amenable to curative surgery. Excluded patients underwent open or laparoscopic surgery. All surgeries were performed by a single surgeon using an SPR device. The operator had at least 3,000 previous single-incision laparoscopic surgery experience. The surgical procedures were right hemicolectomy (RHC), extended RHC (eRHC), left hemicolectomy (LHC), extended LHC (eLHC), and anterior resection (AR). A learning curve was generated using cumulative sum (CUSUM) methodology to assess changes in total operation time (OT), docking time (DT), and surgeon console time (SCT).
OT was defined as the time from skin incision to skin closure. DT was defined as the time from the induction of anesthesia to robot trocar docking. SCT measured the time the surgeon spent using the robot console. If an error occurred during the operation of the machine, the time to re-dock the SPR device was also included. When the robot was difficult to control, surgery was performed using laparoscopic instruments. When the surgical technique changed from SPR to laparoscopy during surgery, it was classified as a laparoscopic hybrid technique. In the case of the laparoscopic hybrid, no additional trocar was inserted for surgery. Three laparoscopic ports were used to connect to handmade glove ports. There were no additional incisions. Postoperative complications were confirmed for surgical site infection, anastomosis leakage, postoperative ileus, postoperative bleeding, urinary retention with foley catheter reinsertion, complications requiring medication, and chylous ascites.
Surgical technique
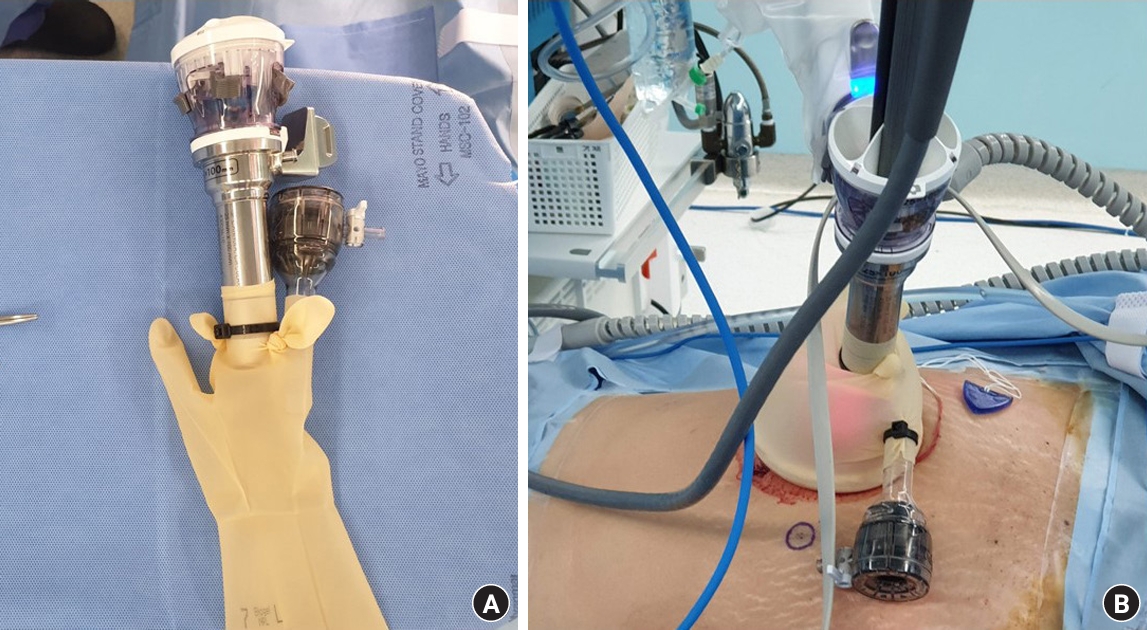
After general anesthesia is performed, the patient is placed with a lithotomy. When the routine drape is completed, a 3- to 4-cm transumbilical incision is made, and a wound protector (Alexis Wound Protector, Applied Medical) is inserted [14]. We used a handmade glove port with surgical latex gloves (Fig. 1). The trocar is fixed using an aseptic cable tie. After CO2 gas is inflated to form a pneumoperitoneum, the position is changed according to the location of the colon cancer to be removed. For cancer on the right side of the colon, reverse Trendelenburg and left-side tilting are performed, and for cancer on the left side of the colon, Trendelenburg and right-sided tilting are performed to facilitate the approach to each major vessel. After the patient’s position is adjusted, the SPR arm and trocar are docked. Next, the robot arms are placed into the abdominal cavity. After identifying the main artery, it is ligated twice using an endoscopic clip (hem-o-lock), and then the resection is performed. For RHC, bowel mobilization is performed with a lateral-to-medial approach. For AR and LHC, a medial-to-lateral approach is used. In addition, after mobilization of the bowel, extracorporeal anastomosis is performed through the incision site. For AR, the distal resection margin was resected using an auto-stapling device. In this case, an additional trocar was used, or resection was performed through the main incision site. End-to-side anastomosis or side-to-end anastomosis is performed using an EEA 25/28 circular stapling device (DST Series EEA stapler, 3.5 mm staples; Covidien) when implementing RHC or LHC. For AR, intracorporeal anastomosis is performed using an EEA 28.
Cumulative sum analysis
For this study, we used a CUSUM analysis to quantitatively express the learning curve. Data were obtained using the mean after sequential arrangement for the OT, SCT, and DT for patients who had SPR surgery for colon cancer. A total of 39 surgical cases were used for this analysis. The CUSUM of the first data point is the difference between that point and the average of all points, and the CUSUM after the second data point checks the difference between the value of the second point and the average of all points added to the accumulation [15]. When the procedure time for each case is defined as Xi, the average procedure time is defined as μ, and the CUSUM of the nth case is sequentially referred to as CUSUMVABPn. The CUSUMVABPn of each case is defined as follows:
The CUSUM graph was expressed using a line chart in Microsoft Excel 2016 (Microsoft Corp). The trend of learning outcomes was confirmed through the slope of the CUSUM curve; where the slope gradually stabilizes after being steep is the breakthrough point of the learning curve. The polynomial curve of the CUSUM table used the trend line function.
Statistical analysis
In addition to the CUSUM schematic, the averages of the continuous variables among the patient characteristics were compared using a 1-way analysis of variance with post hoc Bonferroni correction. Differences in categorical variables were compared using the Pearson chi-square test. Differences with a P-value of less than 0.05 were considered to be statistically significant, and a double test was performed. Microsoft Excel 2016 was used for the CUSUM graph for the learning curve. For statistical processing, IBM SPSS Statistics ver. 25.0 (IBM Corp) was used.
RESULTS
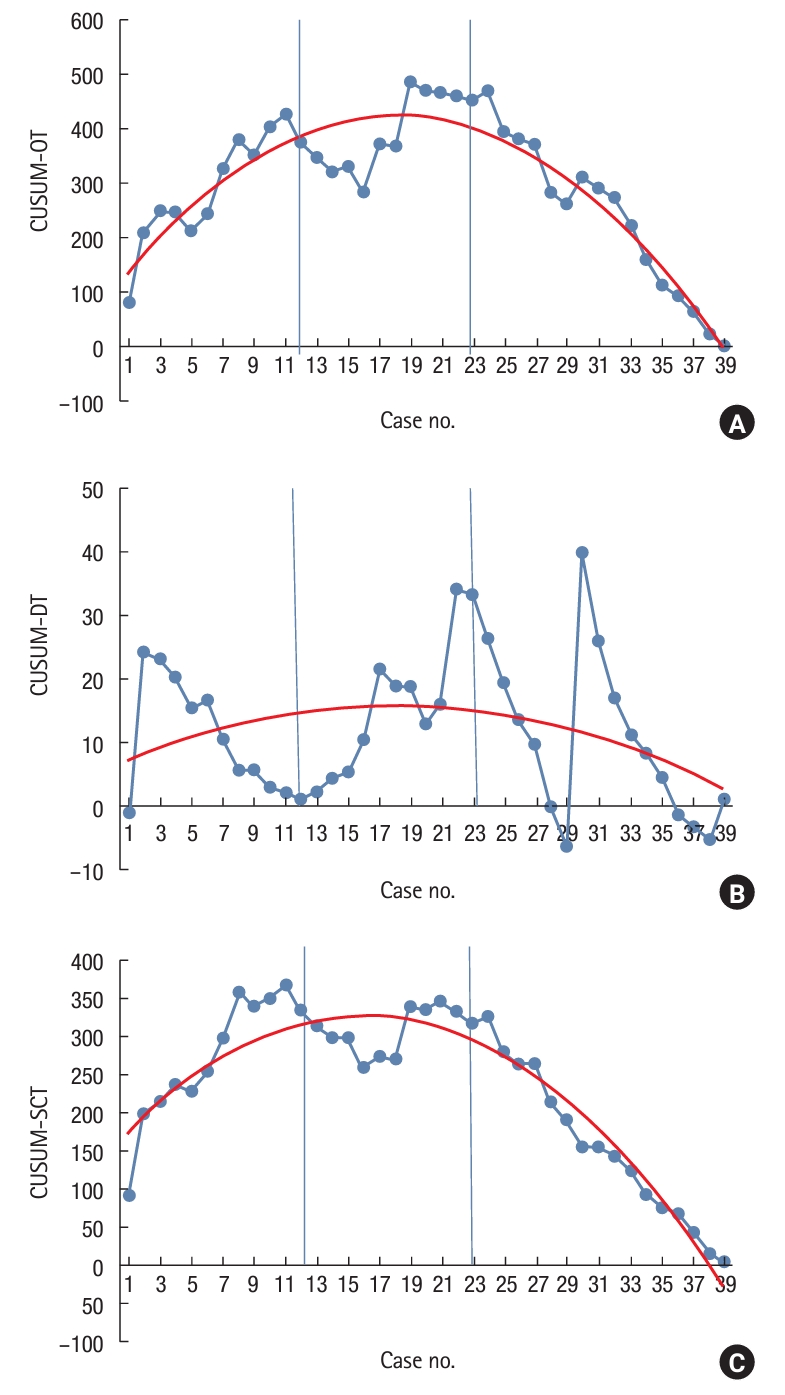
The average age of the patients was 61.28±13.03 years, and they had an average body mass index of 23.79±2.86 kg/m2. Among the patients, 23 were male and 16 were female. The mean American Society of Anesthesiologists (ASA) physical status classification was II. Among the procedures, RHC/eRHC was the most common with 25 cases, followed by AR with 9 cases. By TNM stage, stage III patients were the most common, and the mean tumor size was 4.59±3.34 cm, mean proximal resection margin was 10.97±7.62 cm, and mean distal resection margin was 10.02±10.15 cm; 1 patient had a positive circumferential resection margin. The baseline characteristics of all patients are provided in Table 1. The clinicopathological features of the 39 patients who underwent SPR colectomy did not differ significantly among the phases (Table 1). The mean OT was 186.59±51.30 minutes, and the average SCT was 95.49±35.33 minutes. The average DT was 14.87±10.38 minutes. As shown in Fig. 2, the graphs of all 3 measurement times had negative slopes, indicating that the OT decreased as the number of cases increased. Fig. 3 shows the CUSUM curves. From the first case to the 10th case, the slope is steep, and it flattens out between the 11th and 22nd cases. From the 23rd case, the slope again showed a sharp pattern and then decreased. We classified 3 phases based on those slope changes. The first to 11th cases were defined as phase 1, the 12th to 22nd cases were defined as phase 2, and the 23rd to 39th cases were defined as phase 3. When checking the CUSUM for the learning curve by phase, the OT and SCT differed significantly by phase (Table 2). OT, SCT, and DT were all significantly longer in phase 1 than in phases 2 and 3. In the post hoc test, the OT of phase 1 was significantly longer than the OT of phase 3 (phase 1 vs. phase 2, P=0.203; phase 1 vs. phase 3, P=0.001). Significant differences between phases 1 and 3 were also found in SCT (phase 1 vs. phase 2, P=0.011; phase 1 vs. phase 3, P<0.001); however, DT did not differ among the 3 groups (phase 1 vs. phase 2, P>0.999; phase 1 vs. phase 3, P>0.999). We also checked for differences in surgical methods according to the location of cancer. RHC and eRHC were the most commonly performed surgeries, with a total of 25 cases, and LHC and eLHC were the least commonly performed with 4 cases. Among the types of surgery, AR was the shortest, lasting an average of 132.22 minutes, and LHC and eLHC were the longest at 225.25 minutes. There were 4 cases of laparoscopic hybrid surgery: 0 in phase 1; 2 in phase 2 (19th, 22nd); and 2 in phase 3 (30th, 35th), which were statistically insignificant differences (phase 1 vs. phase 2, P=0.522; phase 1 vs. phase 3, P=0.988; phase 2 vs. phase 3, P>0.999). In particular, in cases 22 and 30, adhesiolysis was performed using laparoscopic hybrid technique before robot docking due to adhesion due to previous surgery.
A total of 8 postoperative complications occurred (Table 3): 2 ileuses, 2 postoperative bleedings, 1 chylous discharge, and 3 urinary retentions. Postoperative complications occurred most commonly in phase 3, with 6, and no complications occurred in phase 2. No patients had a Clavien-Dindo classification grade of III or higher. No mortality or morbidity occurred within 30 days after discharge.
DISCUSSION
Since the introduction of minimally invasive colon cancer surgery using laparoscopy, many technological advances have occurred. One of them is single-incision laparoscopic surgery [8]. Reducing the number of trocars to one minimizes the patient’s wounds, which also has cosmetic advantages and reduces postoperative complications. With the development of robotic technology, robotic surgeries for colon cancer surgery have been developed [16]. An SPR device that combines the advantages of robotics and single-incision laparoscopy was introduced by Intuitive Surgical Inc in 2018. Since that introduction, SPR devices have been used in various fields. Recently, it was confirmed that SPR surgery can be used in gynecology and urology. In urology, prostatectomy was performed using SPR, and in gynecology, the feasibility and safety of SPR for intraperitoneal surgery were verified by performing a hysterectomy using SPR [11, 12]. Its suitability for use in colorectal cancer has also been reported recently. Marks et al. [13] showed the feasibility and safety of left colectomy using SPR.
In this study, we analyzed how many cases must be conducted to achieve proficiency in the new technology. Although many learning curves for robotic surgery have been published, the learning curve for SPR still requires clarification [17–21]. Furthermore, although the learning curve for single-incision laparoscopic colon cancer surgery is well known, no known learning curve for SPR has yet been published [14, 22–24]. We determined the learning curve for SPR colectomy using a CUSUM analysis so surgeons can confirm the degree of convenience offered by SPR and efficiently acquire SPR techniques. Presenting the predicted learning curve for SPR to beginners can improve their access to SPR. Previous studies classified the learning curve into 3 phases to allow it to be checked in detail. We have also classified the learning curve into 3 phases and confirmed the optimal stabilization time.
In this study, we were able to confirm that the surgical performance stabilized 18 surgeries into the learning curve. In previous studies on colorectal surgery, the learning curve stabilized after 15 to 25 cases [17, 18, 21]. Thus, the SPR learning curve does not differ significantly from that for other surgical methods, including laparoscopic surgery [19, 25]. In contrast, when single-incision laparoscopic surgery and conventional laparoscopic surgery are compared, the learning curve for single-incision laparoscopic surgery requires more cases [14]. Although we did not compare the direct learning curve with single-incision laparoscopic surgery in this study, the time to reach a sufficient learning curve for SPR is worth comparing with single-incision laparoscopic surgery. Due to the single-port operation using a robot, various developments have been made compared to the previous laparoscopic surgery. Compared to single-port laparoscopic colectomy, SPR-assisted colectomy has many benefits in reducing learning time. First, compared to single-port laparoscopic colectomy, it can reduce the time and cost of training the scopist. Second, it has the advantage of intuitively and quickly obtaining the required surgical field using the refracted angle view and 3-dimensional focus. Third, depending on the location of the tumor, it is not necessary to additionally consider the incision site.
The reductions in OT and SCT came through decreases in the time required to operate the robot arm, move the camera, and dissect surrounding tissues. A change in docking material after 14 cases further reduced the OT. At the beginning of the operation, the robot was docked using the GelPOINT port (Applied Medical). The GelPOINT port used to fix the trocar applies tension to the incision site. This will limit the movement of the robotic device and interfere with the approach to the intraabdominal organ. To correct that problem, we used a handmade glove port, which we were able to manufacture when preparing for surgery. In that way, we reduced the DT, increased the use of the intraabdominal space, and reduced position restrictions during surgery. A new technique for holding specimens and using gravity for positioning could also reduce the OT. OT, SCT, and DT all differed according to the operation location (Table 4). AR required less OT, SCT, and DT than RHC or LHC because the accessibility of the robot arm for bowel mobilization and main vessel dissection is much easier during AR surgery.
When studying the learning curve for a new skill, the incidence of complications is important. However, in our study, more complications occurred in phase 3 than in phase 1. In phase 3, postoperative ileus, postoperative bleeding, and urinary retention occurred in 6 patients. However, the degree of complication was not serious and did not affect the length of the hospital stay. In phase 3, we enrolled patients with more difficult conditions than in the previous phases, which explains the increase in complications. For example, most of the patients (4 of 6) who experienced complications had a previous operation.
Considering complications following SPR surgery, short-term outcomes should be confirmed. When it was difficult to manipulate the SPR device skillfully during a colectomy, the surgery was performed using a laparoscopic hybrid technique. Laparoscopy was used in 4 surgeries, but the cases did not decrease significantly in the later phases. In the hybrid case in the second phase, laparoscopy was used to reduce the OT. The hybrid cases in phase 3 were in patients with a previous surgical history whose adhesions in the abdominal cavity were severe. No cases of open conversion occurred. The CUSUM learning curve confirms that a surgeon with experience in single-incision laparoscopic surgery needs to complete 17 to 19 SPR surgeries before reaching the top of the learning curve. It is encouraging to consider that the surgeon who participated in this study had no previous experience with robotic surgery.
The major limitation of our study is that we studied the learning curve of only 1 surgeon. Studying the learning curve for several surgeons will help to more accurately calculate the number of cases needed to learn SPR techniques. In addition, the learner’s experience with single-port operations might have caused a left shift in the learning curve; the learning curve for a beginner could be more difficult. Second, only 39 patients were included, which is not a fully enough number for the study. In phase 3, the graph is somewhat flat, but additional results might be obtained if more data had been used. Finally, we tried to analyze differences according to the location of cancer. Surgery for colon cancer differs between RHC and AR. However, the number of patients included in this study was small, so the number of patients receiving each type of surgery was not enough, making it difficult to compare. A larger number of patients would make it possible to subdivide the learning curve and thereby deepen the investigation.
In conclusion, the learning curve for SPR colectomy was completed after 17 to 19 cases. OT and SCT decreased as the number of cases increased. No cases of open conversion were needed, and no severe complications occurred.