INTRODUCTION
Obesity is known to contribute to technical difficulties in performing surgery and postoperative morbidities in laparoscopic colorectal surgery [1–3]. Although, in a systematic review involving 23,649 patients, Hotouras et al. [4] concluded that laparoscopic colorectal resection is safe and technically feasible in terms of postoperative morbidities in patients with obesity, longer operative times in patients with obesity who underwent laparoscopic colorectal surgery have been reported [1, 2, 5–19]. Excessive visceral fat can interfere with finding and maintaining an accurate dissection plane, particularly in minimally invasive surgery [17, 20].
Body mass index (BMI) has been used to measure obesity previously [21]. However, there are reports that BMI does not always correspond to the visceral fat, which can be actually related to short-term postoperative outcomes [22, 23]. Therefore, measurement of visceral fat area (VFA) using computed tomography (CT) has been proposed as an alternative to BMI to more accurately predict short-term postoperative outcomes in laparoscopic colorectal surgery [1, 11, 19, 24, 25]. However, measuring VFA using a CT scan is a time-consuming task and requires the use of specific software; moreover, its cost-effectiveness and usefulness in actual clinical practice is still uncertain [26].
More recently, bioelectrical impedance analysis (BIA) has been used for body composition analysis. This approach uses a simple and noninvasive device that can analyze body composition, such as skeletal muscle mass, water content, and body fat mass, by measuring body resistance and capacitance according to changes in the current [27]. In the present study, we aimed to evaluate the usefulness of a body composition index obtained by using a BIA device to predict the short-term postoperative outcomes in patients undergoing minimally invasive colorectal surgery.
METHODS
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Ewha Womans University Seoul Hospital (No. 2022-04-010). The requirement for informed consent from patients was waived due to the retrospective nature of the study.
Patients
From June 2021 to February 2022, data of patients who underwent elective major colorectal surgery for colorectal cancer using minimally invasive techniques performed by a single surgeon were retrospectively reviewed. Among the 103 patients, those without a BIA index (n=16) and those without follow-up data indicating short-term postoperative outcomes for at least 1 month (n=3) were excluded. In addition, those who had simultaneous resection (n=16) and subtotal colectomy (n=2) were excluded to determine the accurate correlation between body composition index and operative time. Ultimately, the data from 66 patients were included in the study.
Measurement of body composition index
At our institution, patient height and weight are recorded at the time of admission. After bowel preparation on the day before surgery, body composition status is recorded using a commercial BIA device (InBody 270, Inbody Co Ltd) in patients who are scheduled for elective major colorectal surgery. To measure body composition, the patient stands barefoot on a scale and holds the machine’s hand, following simple instructions from the manufacturer. The BIA device used in this study could evaluate body composition and could perform muscle-fat (skeletal muscle mass, body fat mass) and obesity (percent body fat) analyses.
Definition and criteria of the body composition index and prolonged operative time
The surgeries of all enrolled patients were performed by an experienced surgeon with more than 300 cases in performing both laparoscopic and robotic surgeries. In most patients, D3 lymphadenectomy was performed [28]. Data on patients’ characteristics were retrospectively reviewed from the medical records. Operative time, intraoperative blood loss, time to diet, time to gas passing, postoperative hospital stay, postoperative morbidity, and readmission rate within postoperative 30 days, which indicates short-term postoperative outcomes, were recorded. Complications were further classified according to the Clavien-Dindo surgical complication grading system [29]. In cases of robotic surgery, docking time was included in the operative time.
Patients with BMI of ≥25 and <25 kg/m2 were classified into the BMI-high and BMI-low groups, respectively [21]. Patients were further divided according to their body composition index using the mean of the data, because, to our knowledge, there are currently no standard values for body fat mass, percentage body fat, and skeletal muscle mass. In addition, because all of the body composition indexes and operative time showed a normal distribution, the mean value of each variable could be used as the cutoff value. The mean values of body fat mass, percent body fat, and skeletal muscle index were 18.5 kg, 29.1%, and 23.6 kg, respectively. Prolonged operative time was defined as >210 minutes for laparoscopic surgery and >240 minutes for robotic surgery, which was based on the mean value obtained from each group in our study as robotic surgery generally resulted in longer operative times.
Statistics
Continuous variables were compared using the Student t-test and are presented as means with standard deviations or medians with interquartile ranges. Categorical variables were analyzed using the chi-square test or Fisher exact test and are presented as frequencies. A logistic regression model was used to evaluate the factors associated with prolonged operative time. Variables with P-values of <0.10 in univariate analysis were included in a multivariate analysis. Pearson correlation coefficient (r) was used to determine the correlation between operative time and other continuous variables (BMI, body fat mass, percent body fat, and skeletal muscle mass). Receiver operating characteristic (ROC) curve analysis was performed to determine the area under the ROC curve. A P-value of <0.05 was considered statistically significant. All data were analyzed using IBM SPSS ver. 20 (IBM Corp).
RESULTS
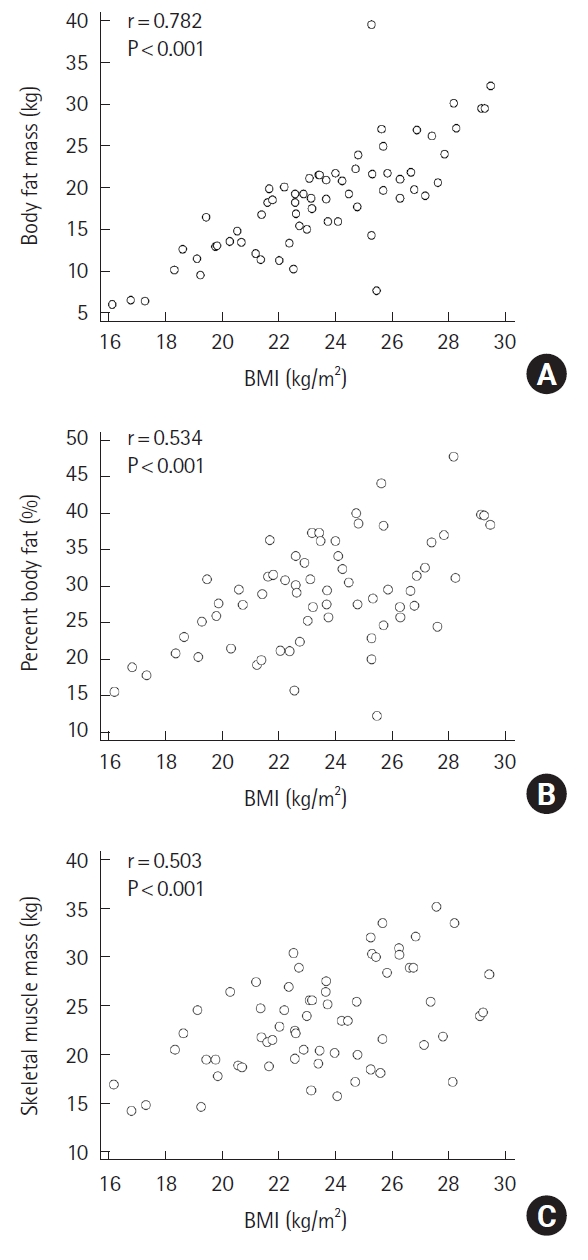
Correlation between BMI and body composition index
In the correlation analysis, positive correlation was observed between BMI and body composition index. Body fat mass was most strongly correlated with BMI (r=0.782, P<0.001). Scatterplots of these associations are shown in Fig. 1.
Patient characteristics and short-term postoperative outcomes according to BMI
Of the 66 patients, 44 (66.7%) were enrolled in the BMI-low group and 22 (33.3%) in the BMI-high group. A comparison of the patient characteristics and short-term outcomes between the groups is shown in Table 1. The mean BMI was 21.8 kg/m² in the BMI-low group and 26.9 kg/m² in the BMI-high group. Patients’ baseline demographics, such as age, sex, American Society of Anesthesiologists physical status grade, Eastern Cooperative Oncology Group performance scale score, and smoking and prior abdominal surgery history, were not significantly different. Among the body composition indexes, body fat mass was significantly higher in the BMI-high group (BMI-low, 15.9±4.6 kg; BMI-high, 23.7±6.6 kg; P<0.001). Tumor location, surgical approach, operative method, and pathological status were not different between the 2 groups. Intraoperative blood loss, time to diet, time to gas passing, postoperative hospital stay, postoperative morbidity, and readmission rates did not differ between the 2 groups. For patients in the BMI-high group, the operative time was prolonged but was not statistically different (BMI-low, 213.6±46.7 minutes; BMI-high, 231.8±48.5 minutes; P=0.146). BMI and body composition index were not associated with complications (Table 2).
Risk factors associated with prolonged operative time
Among the patient characteristics, factors that could be related to operative time were analyzed. In the univariate analysis, body fat mass, percent body fat, tumor location, T category, and N category were associated with prolonged operative time. In the multivariate analysis, percent body fat, tumor location, and status of lymph node metastasis were associated with prolonged operative time (Table 3).
Subgroup analysis according to tumor location, status of lymph node metastasis, and surgical approach between BMI, body composition index, and operative time
A subgroup analysis was performed to identify an accurate indicator of prolonged operative time. In all patients, body fat mass was related to prolonged operative time, although the correlation was weak (r=0.245; P=0.048). There was no correlation between body composition index and operative time in each group according to tumor location. However, in patients with lymph node metastasis, BMI and body fat mass were positively associated with operative time (BMI: r=0.441, P=0.031; body fat mass: r=0.404, P=0.050). In addition, in the robotic surgery group, body fat mass tended to be associated with operative time (r=0.415, P=0.055) (Table 4).
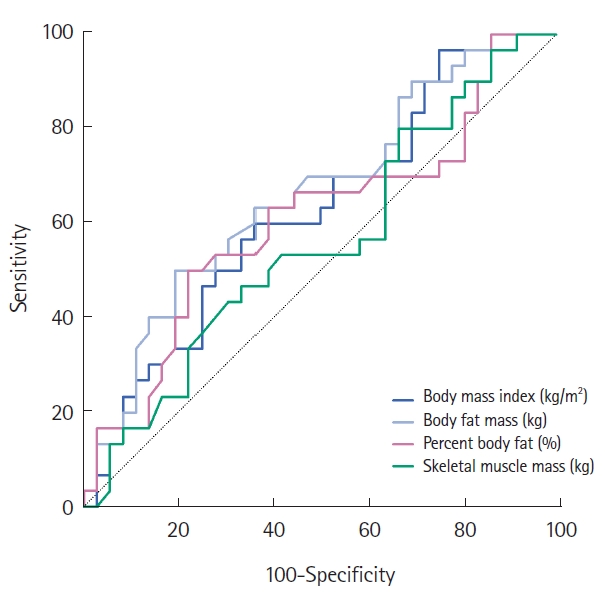
Predictive significance between factors, including BMI, and prolonged operative time with ROC curve analysis
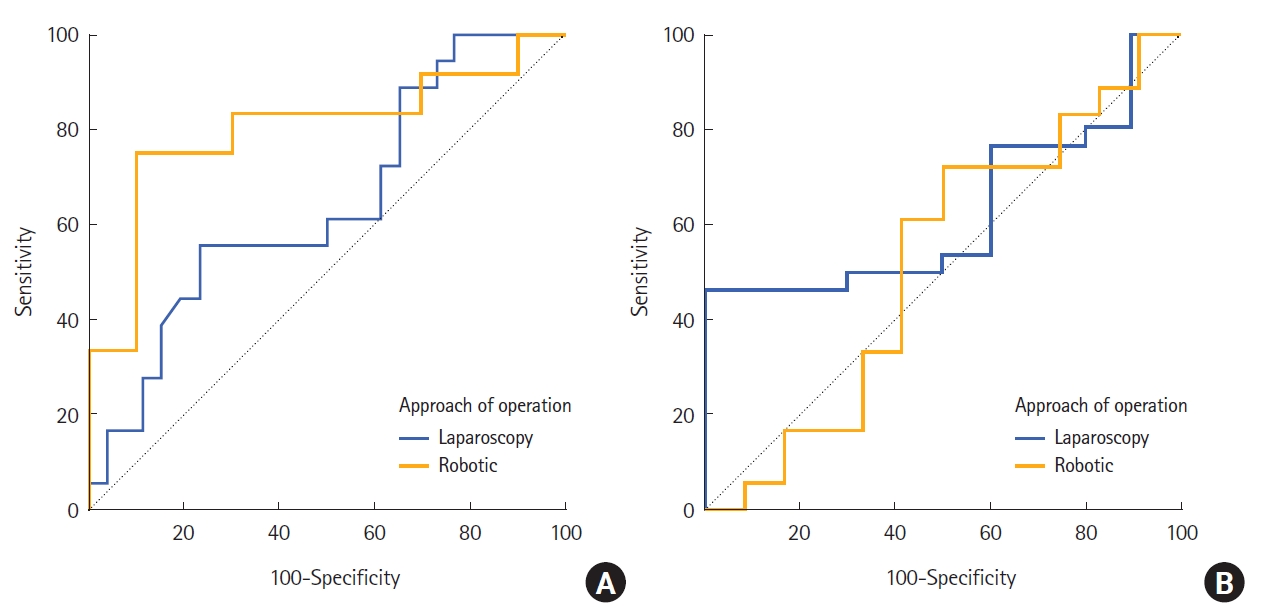
Only body fat mass showed a statistically significant predictive probability for prolonged operative time (body fat mass: area, 0.662; 95% confidence interval, 0.531–0.764; P=0.024). BMI was not a predictive indicator for prolonged operative time (Table 5, Fig. 2). The ROC curves comparing the body fat mass and BMI in the laparoscopic and robotic surgery groups are shown in Fig. 3. Body fat mass was more reliable than BMI in patients who underwent robotic surgery, although it was not statistically significant.
DISCUSSION
In our study, the BIA device, which measures the body composition index, showed a positive correlation with BMI. However, BMI and body composition index were not associated with short-term postoperative outcomes in patients who underwent minimally invasive colorectal surgery. In terms of operative time, percent body fat, among the body composition indexes, was associated with prolonged operative time in the multivariate analysis. In addition, body fat mass was a significant factor for operative time in the ROC curve analysis. The results of this study may suggest that the body composition index with BIA can be used to replace BMI in predicting prolonged operative time.
However, we thought that our data could not demonstrate the usefulness of the body composition index, compared with BMI, in clearly predicting prolonged operative time. Although some factors were significantly related to operative time, the statistical significance was very low and the correlation coefficients were also weak. This could be due to small sample size; however, there is the limitation that body composition index could calculate the entire body fat mass and percent body fat instead of only trunk fat volume which were related with intra-abdominal surgery. The body composition index for predicting prolonged operative time may be used with caution.
We would like to identify more predictive markers of short-term outcomes, other than BMI. BMI is convenient to use, but in actual surgery, visceral fat is more related to intra-abdominal surgery, as compared to BMI, which does not always correspond to the VFA [22, 23]. In addition, the BMI classification, which is used to define obesity, differs between Western and Asian population [21, 22]. Moreover, Asian population have more pronounced abdominal obesity than Europeans, despite both having similar BMI values [30]. Therefore, the VFA analysis using CT scans, which can measure cross-sectional images, has been studied to predict short-term outcomes [1, 11, 19, 24, 25]. However, measuring the area of visceral fat with a preoperative CT scan is also a time-consuming task despite the availability of free programs [26].
Recently, BIA was used to evaluate body composition indices. It is simple, noninvasive, easy to perform, and allows the analysis of other factors, including body fat mass, percent body fat, and skeletal muscle mass. This rapid and cost-effective device can be used repetitively and without any risk [31]. In various fields, there have been many previous studies that utilize the body composition index with a BIA device [32–38]. However, there have been no studies on other indicators of short-term outcomes and operative time using the BIA device, except for skeletal muscle mass, in patients who had undergone colorectal surgery. Shiomi et al. [39] reported that trunk fat volume measured by using a BIA device can be a useful parameter for the evaluation of obesity and a predictor of complications after gastrectomy.
In our study, BMI and body composition index were not associated with short-term postoperative outcomes. Many studies have reported the relationship between obesity and postoperative outcomes. Some surgeons reported the conversion rate to open surgery, anastomotic leakage rate, and complication rate to be greater in patients with obesity than in those without obesity [2, 3]. However, Horouras et al. [4] reported no significant differences in intraoperative blood loss, overall postoperative morbidity, anastomotic leakage rate, reoperation rate, mortality rate, and the number of retrieved lymph nodes between obese and nonobese groups who underwent colorectal surgery in their meta-analysis, which included 17,895 and 5,754 patients without and with obesity, respectively. Our study results were consistent with those obtained by the previous systematic analysis. With the adoption of minimally invasive surgery in general, better results can be achieved with advanced technology and tools, even in patients with obesity.
However, the body composition index has shown promise as a predictive marker for prolonged operative times. The amount of body fat may be more related to prolonged operative time than BMI. Interestingly, the body fat mass was a more reliable predictor of prolonged operative time in patients who underwent robotic surgery than in those who underwent laparoscopic surgery, although the difference was not statistically significant. In patients enrolled in this study, all robotic surgeries were performed with the da Vinci SP (single port, Intuitive Surgical Inc). Visceral fat may more likely affect the operative time in patients undergoing robotic surgery due to the narrow surgical field and absence of an energy device.
This study had several limitations. First, because the analysis was performed retrospectively at a single center, a relatively small number of patients were included. Therefore, definitive conclusions cannot be drawn from this study. Second, this study lacked long-term follow-up data. A study that includes follow-up data collected using BIA after surgery is necessary to determine the relationship between body composition status and long-term outcomes. However, to the best of our knowledge, our study has an advantage, as we were able to identify the correlation between the body composition index and operative time in patients undergoing minimally invasive colorectal surgery using a noninvasive, reliable, and reproducible device.
In conclusion, the body composition index measured by using a BIA device can be a reliable marker for predicting prolonged operative time, instead of BMI, even though it did not show a difference in short-term outcomes. The body composition index can be used as a predictive marker for prolonged operative time.