INTRODUCTION
The incidence of colonic diverticulitis is increasing, both in Asian and Western countries. This increase may be due to improvements in diagnostic tools, such as abdominopelvic computed tomography (CT), which can provide detailed diagnosis of diverticulitis between different variants of disease progression [1,2]. Diverticulitis can be classified as uncomplicated or complicated using a CT evaluation. Uncomplicated diverticulitis is characterized by evidence of colonic wall thickening or pericolic inflammatory changes whereas complicated diverticular disease is characterized by the presence of abscesses, fistulas, obstructions, and/or localized or free perforations. The severity of acute diverticulitis is often graded by using the modified Hinchey classification [1,2,3,4]. Surgical management of diverticulitis has been questioned, with conservative management increasingly being used in patients with diverticulitis in both the right and the left colon. Moreover, surgery may not always be appropriate in patients with a complicated form of diverticulitis.
Few studies to date have compared the managements of patients with diverticulitis in the right and the left colon. This study evaluated the management of diverticulitis as a function of disease location (right or left colon) and disease severity (complicated or uncomplicated). In addition, factors associated with complicated diverticulitis were determined.
METHODS
Patients diagnosed with colonic diverticulitis by using abdominopelvic CT at Chonbuk National University Hospital, South Korea, from 2007 to 2014 were retrospectively evaluated. Demographics and clinical features, including age, sex, results of physical examinations, body mass index (BMI), comorbidities, changes in bowel habits, length of hospital stay, duration of antibiotic use and bowel rest, CT findings, type of surgery, and disease recurrence, were obtained from patients' records. Abdominopelvic CT findings were categorized by using the modified Hinchey classification, with patients classified as having stages Ib, II, III, and IV diverticulitis, as well as fistula or obstruction, being defined as having complicated diverticulitis [2]. Patients without CT scan evidence of diverticulitis were excluded from the study. Categorical variables were compared by using the chi-square and Fisher exact tests whereas continuous variables were compared by using Student t-tests. A logistic regression analysis was used for the multivariate analysis. Results with P-values < 0.05 were considered statistically significant.
RESULTS
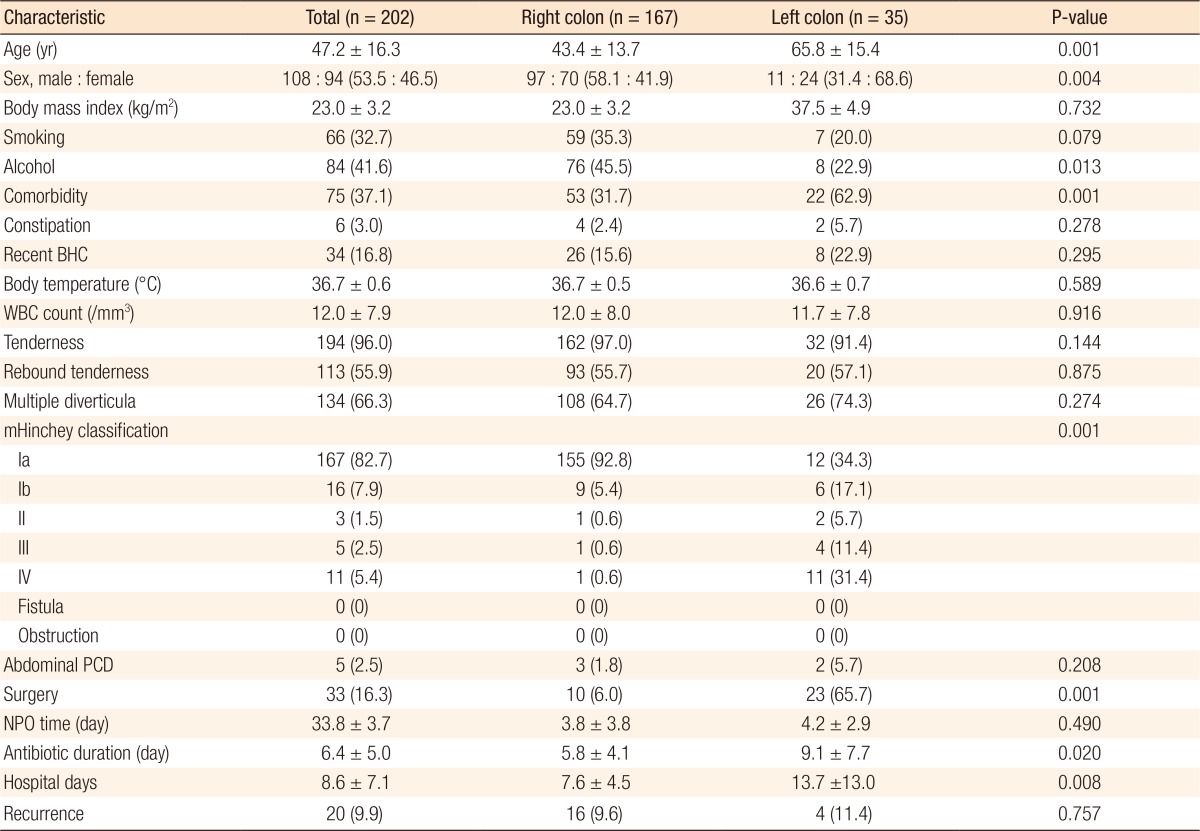
During the study period, 202 patients, 108 males (53.5%) and 94 females (46.5%), were diagnosed with diverticulitis, including 167 patients (82.7%) with right-sided and 35 (17.3%) with left-sided colonic diverticulitis. Patients with right-sided diverticulitis were significantly more likely to be younger (43.4 ± 13.7 years vs. 65.8 ± 15.4 years, P = 0.001) and to be male (58.1% vs. 31.4%, P = 0.004), but significantly less likely to have comorbidities (31.7% vs. 62.9%, P = 0.013), than patients with left-sided diverticulitis. Other variables in these 2 groups are shown in Table 1, and the results of the multivariate analysis of factors significantly associated with the location of diverticulitis are shown in Table 2.
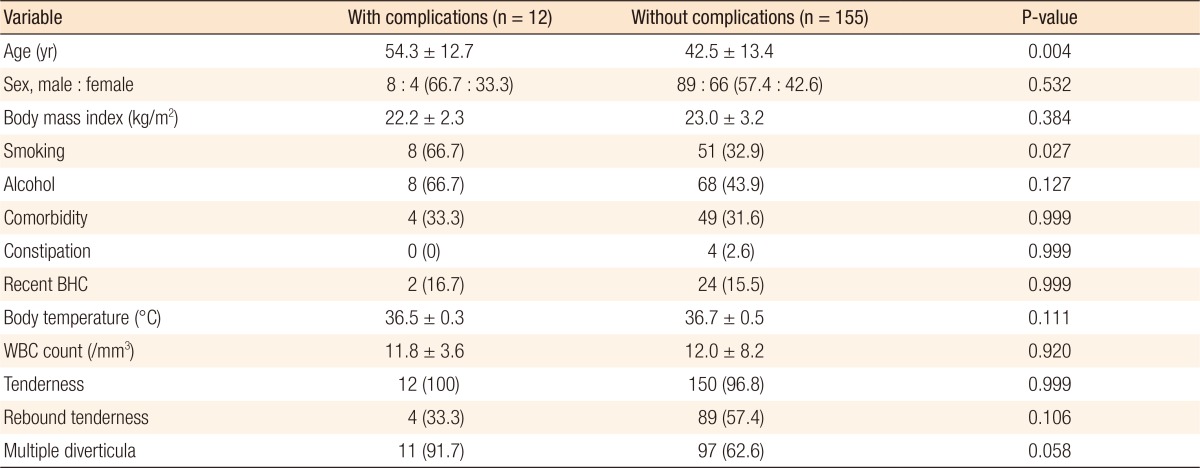
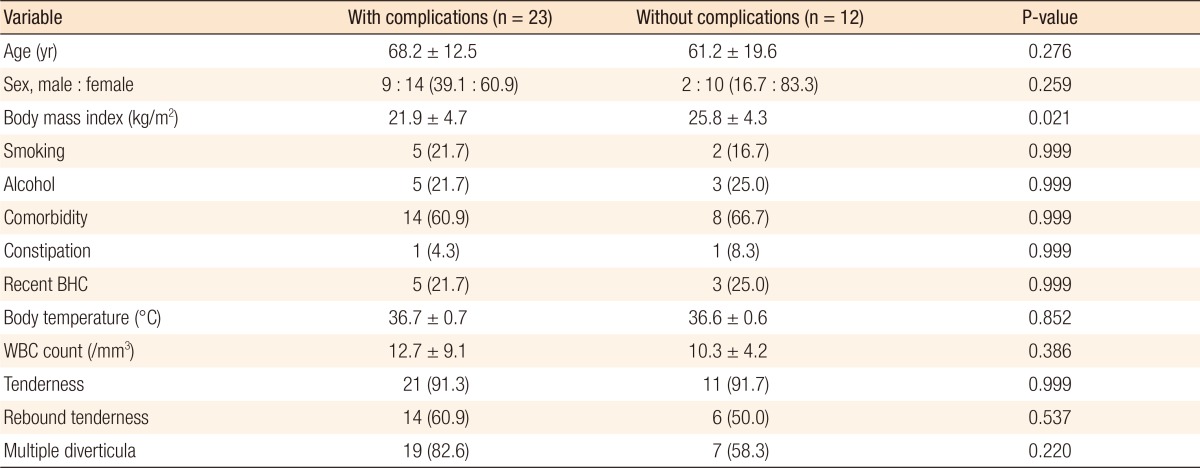
Statistical analysis showed that factors significantly associated with complicated diverticulitis were dependent on disease location. Compared with patients with uncomplicated right-sided diverticulitis, those with complicated right-sided diverticulitis were significantly more likely to be older (54.3 ± 12.7 years vs. 42.5 ± 13.4 years, P = 0.004) and to be smokers (66.7% vs. 32.9%, P = 0.027) (Table 3). However, among patients with left-sided diverticulitis, those with complicated disease had significantly lower BMI (21.9 ± 4.7 kg/m2 vs. 25.8 ± 4.3 kg/m2, P = 0.021) than those with uncomplicated disease (Table 4).
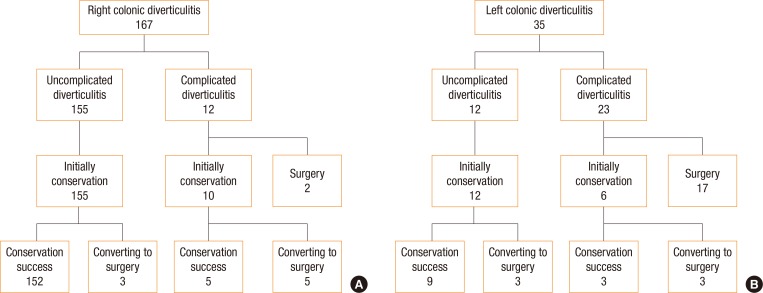
Of the 172 patients with right-sided disease, 12 (7.2%) had complicated and 155 (92.8%) had uncomplicated diverticulitis. Of the 12 patients with complicated diverticulitis, 7 were managed surgically, and 5 were managed conservatively. Of the 155 patients with uncomplicated diverticulitis, 152 were successfully managed conservatively. The other 3 patients were initially managed conservatively, but eventually underwent surgery (Fig. 1A).
Of the 35 patients with left-sided disease, 23 (65.7%) had complicated and 12 (34.3%) had uncomplicated diverticulitis. Of the 23 patients with complicated diverticulitis, 17 were managed surgically, and 6 were initially managed conservatively. Three of the latter 6 patients, however, failed conservative management and eventually underwent surgery. Of the 12 patients with uncomplicated diverticulitis, 9 were successfully managed conservatively, with the remaining 3 patients requiring surgery (Fig. 1B).
DISCUSSION
This retrospective analysis suggests that management of patients with colonic diverticulitis is dependent on both disease location and severity. This analysis also identified clinicopathological factors associated with both disease location and disease severity.
The demographic and the clinical characteristics of the patients in the present study were similar to those in previous studies of diverticulitis. Right-sided colonic diverticulitis has been reported to occur predominantly in relatively young males whereas left-sided diverticular disease is more common in women, with its incidence increasing with age [5,6,7,8,9]. The present study also found that left-sided colonic diverticulitis was significantly associated with both older age and female sex.
Diverticulitis in younger patients (<50 years) has been described as more virulent and more likely to be associated with complications [10,11]. In addition, smoking was found to be a risk factor in patients with symptomatic disease and to be related to complications [12,13]. The present study found that older age and smoking were significantly associated with complicated right-sided diverticulitis whereas low BMI was significantly associated with complicated left-sided diverticulitis. To our knowledge, no previous study has assessed factors associated with locations of complicated diverticulitis from the same population. The findings of this study suggest that special considerations may be required to manage patients with factors associated with complicated diverticulitis. These patients initially have uncomplicated diverticulitis, which becomes aggravated and complicated, resulting in a switch from conservative to surgical management. Additional large scale studies are required to confirm these findings, especially in patients with complicated left-sided diverticulitis.
Conservative management has been shown to be effective in patients with uncomplicated diverticulitis, both in the right and the left colon [14,15,16,17,18,19]. However, the optimal treatment of complicated diverticulitis has not been determined as improvements in surgical techniques and medical management have led to changes in management. Traditionally, most patients with complicated diverticulitis have been managed surgically, by, for example, resection of the perforated segment of the colon [20,21,22,23]. Conservative management of complicated diverticulitis has been reported to be successful [24,25]. Medical management in patients with complicated diverticulitis may have the goal of converting an emergency surgery to an elective one [2,26,27].
The results of the present study suggest that conservative management may be effective in patients with right-sided colonic diverticulitis. Of the 155 patients with uncomplicated right-sided diverticulitis, 152 (98%) were treated conservatively, and only 12 of the 167 patients (7%) with right-sided diverticulitis had complicated disease. Of those 12 patients, only 2 required emergency surgery for acute peritonitis and sepsis. Three patients with uncomplicated and 5 with complicated right-sided diverticulitis were initially managed conservatively, but eventually underwent a right hemicolectomy. A review of the medical records and the radiologic findings could not identify any criteria or indications for surgery in these patients, suggesting that these patients may have undergone unnecessary surgery that had been performed at the discretion of a surgeon not specializing in colorectal surgery. Those patients likely could have been managed conservatively.
Because the number of patients with left-sided colonic diverticulitis was relatively small, we could not determine any effective treatment modality. Our findings suggest, however, that conservative management may be effective for patients with uncomplicated diverticulitis, but that surgical management may be better for patients with complicated diverticulitis. Of the 23 patients with complicated left-sided diverticulitis, 20 (87%) underwent surgery, with 15 having Hinchey stage III or IV disease requiring emergency surgery.
This study had several limitations, including its retrospective design and its performance at a single tertiary center where almost all patients were Asian. Moreover, only inpatients were included; no outpatients had mild diverticulitis. Therefore, this study was limited in assessing the clinical features of all patients diagnosed with diverticulitis. In addition, the number of patients with left-sided diverticulitis was much smaller than the number with right colonic-sided diverticulitis. Finally, this study did not evaluate the long-term effects of conservative management of diverticulitis, specifically the recurrence rate.
In conclusion, conservative management may be effective in patients with right-sided colonic diverticulitis, whether complicated or uncomplicated, and in patients with uncomplicated left-sided diverticulitis. Patients with complicated left-sided diverticulitis may, however, require surgical management. In addition, special attention should be paid in managing patients with factors associated with complications, such as older age and smoking in patients with right-sided and low BMI in patients with left-sided complicated diverticulitis.