INTRODUCTION
An endometrial stromal sarcoma (ESS), an uncommon uterine mesenchymal neoplasm, accounts for approximately 0.2% of all uterine malignancies [1]. Its occurrence at extrauterine sites is very rare, but it has been reported to occur at the ovary, bowel wall, abdomen, peritoneum, pelvis, and vagina [2]. Primary gastrointestinal involvement is rare [3,4,5,6,7,8,9,10,11,12,13]. We hereby present a case of a primary low-grade extrauterine ESS (EESS) in the sigmoid colon with a review of the literature. No evidence of a primary uterine ESS was found.
CASE REPORT
A 52-year-old woman was transferred from an outside clinic in order to evaluate the bloody stool and a pedunculated mass in the sigmoid colon that had been detected in a rigid sigmoid-scope examination. She was suffering from constipation, unspecified abdominal pain and hematochezia for a month. Her past and family histories were all unremarkable. Laboratory findings were unremarkable, except for mild anemia.
Colon fiberscopy was performed and revealed a fungating mass obstructing the lumen at the distal sigmoid colon (20 cm from the anal verge) (Fig. 1A). Under the impression of colon cancer, a biopsy was taken and suggested the possibility of a gastrointestinal stromal tumor (GIST) showing uncertain malignant potential. Abdominal computed tomography showed an eccentric and irregular wall thickening with enhancement measuring about 5 cm and perirectal lymph node enlargement (T3 or T4aN1M0, stage IIIB) (Fig. 1B). A laparoscopic low anterior resection was carried out, and an umbilicated polypoid mass measuring about 3.8 cm ├Ś 2.5 cm was identified in the distal sigmoid colon; on serial sections, it was found to have infiltrated the mesocolic fat (Fig. 1C, D). No dilation of the proximal bowel side to the mass was identified.
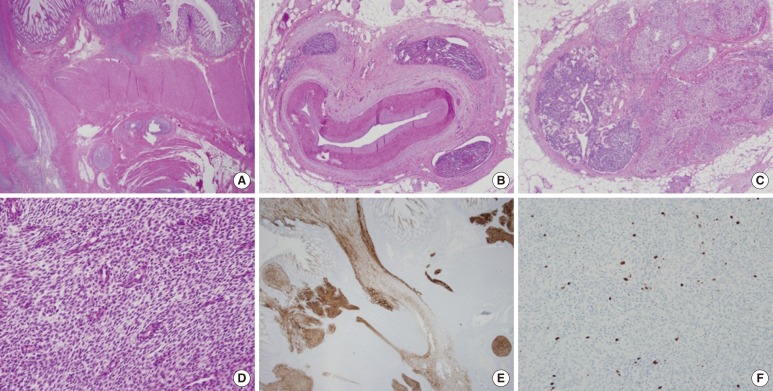
On histopathologic findings, the tumor showed geographic sheets or nests expanding to or infiltrating into the proper muscle and mesocolic fat (Fig. 2A), extensive lymphovascular invasion (Fig. 2B), and metastasis to regional lymph nodes (Fig. 2C) and to the pelvic peritoneum. In spite of extensive sampling, no focus of endometriosis was found in the resected colon specimen. Uniformly small, bland tumor cells with rounded-ovoid nuclei, evenly dispersed chromatin, no or inconspicuous nucleoli, and scanty cytoplasm with indistinct cell borders were noticed (Fig. 2D). Small, prominent arterioles were scattered among the stromal tumor cells. No mitosis or necrosis was identified. The tumor cells were strongly and diffusely immunoreactive for CD10 (1:50, Novocastra, Newcastle, UK) (Fig. 2E), estrogen receptor (ER; 1:40, Novocastra), and progesterone receptor (PR; 1:200, Novocastra), but negative for c-kit (1:600, Dako, Carpinteria, CA, USA), CD34 (predilution, Novocastra), Dog1 (1:500, Dako), ╬▒-smooth muscle actin (1:100, Novocastra), S100 protein (1:200, Novocastra), desmin (1:50, Dako) and pan-cytokeratin (1:200, Novocastra). The Ki-67 (1:100, Dako) labeling index was 8% (Fig. 2F).
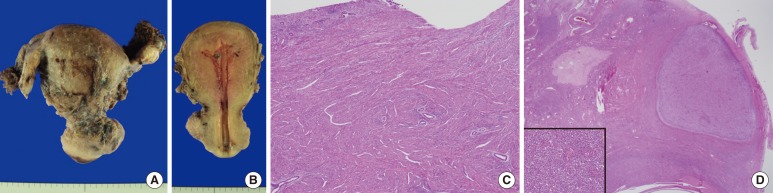
Endometrial curettage was conducted postoperatively and showed secretory hyperplasia and no evidence of ESS. Two months later, a total abdominal hysterectomy with a bilateral salpingo-oophorectomy was performed. The uterus measured 6.0 cm ├Ś 10.0 cm ├Ś 4.5 cm, and upon cross section, the uterine wall was thickened up to 3.2 cm and revealed an ill-defined trabeculated area with several hemorrhagic foci and a myomatous mass in the low uterine segment (Fig. 3A, B). Microscopically, it was diagnosed as adenomyosis, an intramural leiomyoma, and a relatively atrophic endometrium (Fig. 3C). Grossly, the bilateral adnexae were unremarkable, but microscopic foci of the endometrial stromal nodule were identified in the right and left ovaries and measured 0.6 cm and 0.8 cm, respectively (Fig. 3D). However, no focus of endometriosis was found in the uterus or bilateral adnexae. The patient was alive four months after the resection with no evidence of recurrence.
DISCUSSION
An ESS arising outside the uterus at extraovarian sites in the absence of a primary uterine lesion is extremely rare, and only several case reports are present in the English literature. The abdomen and the pelvis are the most common locations for an EESS, and its occurrence in the colonic wall is exceedingly rare, with only 9 reported cases in the literature (Table 1) [4,5,6,7,8,9,10,11]. Together with our case, 10 cases of an EESS in the colon have been reported, and the ages of the patients ranged from 38 to 80 years (mean, 52.2 years). The symptoms at presentation were abdominal pain, difficult defecation, hematochezia and alteration of bowel habits. The sigmoid colon and rectum are the most common sites of occurrence (9 out of 10 cases), which reflects the areas of the bowel having the highest incidence of endometriosis and the anatomic proximity to the ovary. Local dissemination was discovered at the time of the colonic resection in 8 out of the 10 cases, but no recurrence, except for one case, was found during the follow-up period (4 months to 4 years).
Associated foci of endometriosis in the colonic wall, peritoneal cavity or other sites were documented in 8 out of 9 previously reported cases. In our case, in spite of extensive sampling, no histological evidence of endometriosis was found in the specimens of the resected colon and both ovaries. Because the foci of endometriosis are almost always present in the vicinity of the EESS, one suggest that the primary EESS probably originated from an ectopic endometrial stroma of endometriosis, but our case implies that the mere absence of endometriosis does not preclude a primary EESS at that site. The pathogenesis of a primary EESS with no evidence of endometriosis is indefinite. The possibility is mentioned that the tumor might have originated from gland-poor foci of endometriosis [2], de novo from the peritoneal surface or the coelomic or subcoelomic multipotential epithelium [14, 15].
Malignant transformation is a rare, but well-known, complication of endometriosis, and most of these malignant neoplasms are endometrial adenocarcinomas (EAs). Yantiss et al. [11] reported 17 cases of gastrointestinal endometriosis complicated by neoplasms or precancerous changes. The neoplasms comprised 8 cases of EA, 4 cases of a M├╝llerian adenosarcoma, one case of an endometrioid adenofibroma of borderline malignancy with a carcinoma in situ, and one case of an EESS.
An unexpected location and an unusual presentation of an EESS may make the diagnosis challenging, despite classic histologic features. The GIST is the main differential diagnosis in the cases of an EESS arising in colon. The typical spiral arteriole-like vessels and perivascular whorl arrangement of monotonous spindle tumor cells should raise suspicion of an ESS. Immunohistochemistry is useful to distinguish these two entities. A GIST is known to be positively immunoreactive for c-kit, but an ESS is not. Moreover, an ESS shows diffuse immunoreactivity for CD10, ER, and PR. In our case, the tumor cells were strongly and diffusely immunoreactive for CD10, ER, and PR, but negative for c-kit.
In summary, we report a rare case of a primary EESS arising in the sigmoid colon in a 52-year-old woman with local dissemination to the pelvic peritoneum and both ovaries. Endometriosis was not found in specimens of the resected colon and both ovaries.