INTRODUCTION
Colonoscopy is a commonly performed procedure for the diagnosis and treatment of a gastrointestinal disease. Complications after a colonoscopy are rare, with perforation and hemorrhage being the most frequent [1, 2]. Acute cholecystitis after a colonoscopy is a rare event, and no case has been reported to date in Korea. We report a case of acute cholecystitis after a colonoscopy.
CASE REPORT
A 35-year-old male underwent a screening colonoscopy. A 5-mm-sized sessile polyp was noted in the sigmoid colon. After informed consent had been obtained, an uneventful hot snare polypectomy was performed. About 48 hours after the procedure, the patient visited the emergency room with epigastric pain. Physical examination revealed right upper quadrant and epigastric tenderness. The patient had a blood pressure of 150/90 mmHg, a heart rate of 105 beats/min, a respiratory rate of 22 times/min, and a body temperature of 38.5Ōäā. Peripheral blood tests showed white blood cell, 13,300 mm2; neutrophils, 75.0%; hemoglobin, 17.0 g/dL; and platelets, 309,000 mm2. Blood biochemistry showed total bilirubin 1.7 mg/dL; serum glutamic oxalacetic transaminase, 42 IU/L; serum glutamic pyruvic transaminase, 115 IU/L; alkaline phosphatase, 263 IU/L; blood urea nitrogen, 5.9 mg/dL; creatinine, 1.1 mg/dL; and C-reactive peptide, 29.3 mg/dL.
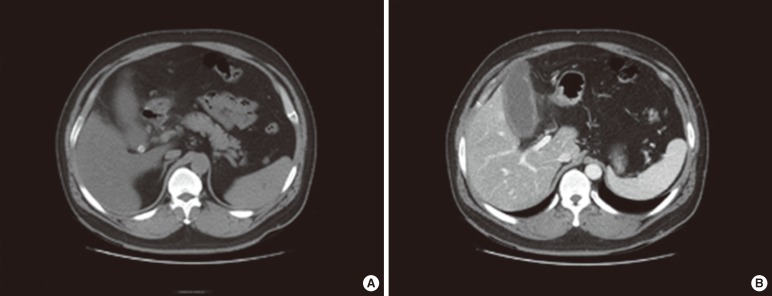
On a plain radiograph, no intraperitoneal air was seen. Abdominal computed tomography showed a 1-cm-sized gallstone in the gallbladder neck, which had a thickened wall and pericholecystic inflammation (Fig. 1). The patient was treated with intravenous antibiotics, and his symptoms and lab findings were improved within 3 days. He was discharged 7 days after admission and was given oral antibiotics; he planned to undergo a cholecystectomy.
DISCUSSION
Complications after a colonoscopy are rare, and perforation is the most common complication of this procedure. The rate of perforation reported in large studies is 0.3% or less and is generally less than 0.1% [3]. The second most common complication is hemorrhage, and other miscellaneous complications of a colonoscopy include splenic rupture, acute appendicitis, diverticulitis, subcutaneous emphysema, and tearing of mesenteric vessels with intraabdominal hemorrhage. Acute cholecystitis after a colonoscopy was first reported by Milman and Goldenberg [4]. All patients of the 8 cases reported in the literature had uneventful routine colonoscopies and developed cholecystitis within 72 hours after the procedures. Seven of them had concurrent cholelithiasis, and all patients recovered uneventfully after a cholecystectomy. All cases reported in literature are summarized in Table 1.
Some hypotheses have been suggested in the previous literature about the cause of acute cholecystitis after a colonoscopy. The relative dehydration caused by bowel preparation may make the patients more susceptible to developing acute cholecystitis. Dehydration caused by bowel preparation may lead to bile stasis, increased bile lithogenicity, and gallbladder distention, which increase the risk of a local inflammatory reaction [4]. In this setting, a preexisting gallstone can become impacted in the gallbladder neck or in the cystic duct [5], contributing to cholecystitis. Other proposed mechanisms are mechanical manipulation associated with bacterial translocation of the colon, and trauma or an adjacent inflammatory response from a polypectomy [4, 6, 7].
Our patient had an uncomplicated, uneventful colonoscopy and developed cholecystitis 48 hours after the procedure. The patient likely had a longstanding asymptomatic gallstone that became symptomatic after the colonoscopy. Transient relative dehydration caused by bowel preparation may have made the bile more concentrated so that the preexisting stone became impacted in the gallbladder neck, leading to acute cholecystitis.
Although the reason our patient developed cholecystitis is not clear, the clinical characteristics and course of our case are correlated with those in the previous literature. While acute cholecystitis after a colonoscopy is a rare complication, we should consider cholecystitis in the differential diagnosis of postcolonoscopy abdominal pain and fever once common complications have been excluded.