Predisposing factors for high output stoma in patients with a diverting loop ileostomy after colorectal surgeries
Article information

Abstract
Purpose
One of the most common ileostomy-related complications is high output stoma (HOS) which causes significant fluids and electrolytes disturbances. We aimed to analyze the incidence, severity, and risk factors for readmission for HOS.
Methods
We reviewed all patients who underwent loop ileostomy closure in a single institution between 2010 and 2020. Patients that were readmitted for dehydration due to HOS during the time interval between the creation and the closure of the stoma were identified and divided into a study (HOS) group. The remaining patients constructed the control group.
Results
A total of 307 patients were included in this study, out of which, 41 patients were readmitted 73 times (23.7% readmission rate) for the HOS group, and the remaining 266 patients constructed the control group. Multivariate analysis identified; advanced American Society of Anesthesiologists (ASA) physical status (PS) classification, elevated baseline creatinine, and open surgery as risk factors for HOS. Renal function worsened among the entire cohort between the construction of the stoma to its closure (mean creatinine of 0.82 vs. 0.96, P<0.0001).
Conclusion
Loop ileostomy formation is associated with a substantial readmission rate for dehydration as a result of HOS, and increasing the risk for renal impairment during the duration of the diversion. We identified advanced ASA PS classification, open surgery, and elevated baseline creatinine as predictors for HOS.
INTRODUCTION
The construction of a diverting loop ileostomy (DLI) is frequently utilized as a means for fecal diversion during operations at increased risk for anastomotic leak, the most of which is restorative proctectomy for rectal cancer, where fecal diversion helps in minimizing the morbidity associated with anastomotic leak [1, 2].
However, the creation of a DLI involves its own perioperative and postoperative complications [3]. Among the most common complications which cause readmissions following the creation of an ileostomy are disturbances in fluid balance, acid-base balance, and electrolytes abnormalities. A normally functioning ileostomy secretes up to 1,000 mL of fluid which includes sodium, chloride, bicarbonate, and potassium, and thus may result in a state of ongoing dehydration. Most of the patients adapt to the new situation by anatomical and endocrine changes, the main modification being the renin-angiotensin-aldosterone system which helps absorb the sodium through amiloride-sensitive-epithelial-sodium channels located along the small bowel mucosa [4–7]. Impairment in those adaption mechanisms and other factors (such as infectious, mechanical, medications) could result in an imbalance and cause high output stoma (HOS). HOS is a complication unique to small bowel stoma, which can cause dehydration, and acute kidney injury. The effluent from HOS usually becomes clinically significant when the daily output exceeds 2,000 mL [8] leading to water, magnesium, and sodium depletion, and malnutrition and failure to thrive later on. Studies have shown that at least 20% of the patients with HOS presented with a significant decrease in glomerular filtration rate (GFR) following creation of an ileostomy compared to their preoperative values [9, 10]. Although early closure of the ileostomy may improve renal prognosis, in 17% of the patients who underwent ileostomy closure, renal function worsened following ileostomy closure [11]. Recurrent episodes of acute renal failure are related to long-term renal prognosis; therefore, the prevention of these acute events of renal failure has a substantial prognostic importance. The reported incidence of HOS varies between 1% and 17% and it is the cause for 4% to 43% of readmissions of patients with an ileostomy [12, 13]. Although the exact cause is unknown, multiple possible factors are thought to contribute to the development of HOS, among which are intraabdominal infections, bowel obstruction, enteritis, short bowel, sudden drug withdrawal (opioids, steroids), or administration of prokinetic drugs (metoclopramide) [14, 15].
The aim of this study was to analyze the frequency and severity of HOS-related readmissions among patients who underwent a DLI creation. In addition, we seek to establish perioperative risk factors for the later development of HOS in order to prevent HOS by early intervention protocols.
METHODS
Ethics statements
This study was approved by the Institutional Ethical Committee of The Chaim Sheba Medical Center (Helsinki Committee, No. 7743-20). The informed consent was waived by the Committee.
Study design
This is a retrospective review of all patients who underwent DLI closure at a single tertiary hospital (The Chaim Sheba Medical Center, Tel Hashomer, Israel) between 2010 and 2020. The DLI was usually constructed 20 to 30 cm away from the ileocecal valve. All readmission cases were recorded. For analysis of the current study, only readmission due to dehydration and HOS during the time interval between the DLI construction and its closure was considered an event. Readmissions for reasons other than dehydration and HOS (e.g., infection, ileus) were not included in the study. Patients presenting with HOS-related readmission were included in the study (HOS) group. HOS was defined as any readmission due to clinical or laboratory signs of dehydration together with patients’ self-reports of increased stoma output. Since most of those patients haven’t accurately recorded the stoma outputs, we don’t have the data on the stoma amount. All other patients with DLI were included in the control (non-HOS) group.
Outcome measures
Patients’ characteristics included demographics, American Society of Anesthesiologists (ASA) physical status (PS) classification, body mass index (BMI), patients’ comorbidities, smoking status, diagnosis and indication for stoma at the time of initial surgery, preoperative treatments (steroid, biologics, anticoagulation, and radiotherapy), surgical approach of initial surgery (laparoscopy vs. open), adjuvant chemotherapy, and time interval between the construction of the DLI to its closure.
In order to assess for chronic kidney injury as a result of the DLI formation, we compared serum creatinine level at the time of the index surgery to the serum creatinine level at the time of stoma closure. The creatinine ratio was defined as creatinine level at the time of stoma closure divided by the creatinine level at the index surgery.
Main outcome measures were number of readmissions due to HOS, serum creatinine level (normal range, 0.51–0.95 mg/dL), presence of sodium (normal range, 136–148 mEq/L) or potassium (normal range, 3.5–5.2 mEq/L) abnormalities, and the length of hospital stay (LOS) during readmission.
Statistical analysis
Data analysis was performed using IBM SPSS ver. 25 (IBM Corp) with a 2-sided significance level of α= 0.05. Descriptive statistics are presented using prevalence and percentage values for categorical variables, while continuous variables are presented with means and standard deviation, skewed distributed variables are presented by median and range.
Group comparisons used the Student t-test for continuous normally distributed variables, and the Mann-Whitney test for a parametric comparison. Categorical comparisons used the chisquare test, Fisher exact tests.
Univariate analysis was performed using a univariate binary logistic regression, multivariate analysis including only the univariate significance variables, was performed by binary logistic regression model with forward likelihood ratio method to exclude nonsignificant variables from the model. A binary logistic regression model was built by model fit method, including the categorical variables as factors and the continuous variables as co-variants.
RESULTS
Demographics and clinical data
A total of 307 patients were included in this study, out of which 41 patients (13.3%) presented with readmissions due to dehydration and HOS (HOS group), and the remaining 266 patients comprised the control group. The HOS group had a mean age of 64.02 years old compared with a mean of 59.7 years among the control group (P= 0.014). There were no significant differences between the groups in terms of sex (56% of males), and mean BMI (25.6± 4.7 kg/m2) (Table 1). The HOS group had significantly more patients with diabetes mellitus (31.7% vs. 15.4% in the control group, P=0.011), more patients with chronic kidney disease (17.1% vs. 1.1%, respectively; P< 0.0001), and more patients treated with steroids (7.3% vs. 0.4%, respectively; P= 0.008).

Demographics and preoperative data
The most common diagnosis and indication for the index surgery was colorectal cancer (80.8%), with the rest being mainly inflammatory bowel disease (IBD), diverticulosis, and familial adenomatous polyposis. The most common index surgery was low anterior resection of the rectum (71.3%), with the rest being mainly cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) (8.8%), total proctocolectomy with ileal pouch-anal anastomosis (4.2%), and ileocolic resection (1.6%) (Table 2). While 36.5% of the index surgeries were done by laparoscopy, 63.5% were done via an open laparotomy. The HOS group index surgeries laparoscopy rates were lower compared with the control group (19.5% vs. 39.1%, respectively; P= 0.015).

Clinical operative data and kidney functions
The vast majority of DLI (86.0%) were performed electively during the index surgery in order to temporarily protect a distal anastomosis while 9.1% were done as part of an urgent surgery due to anastomotic leakage with no significant differences between the 2 groups.
Subgroup analysis of only the 204 patients who had the stoma created electively during a low anterior resection for rectal cancer has showed the same results. Twenty-eight patients (13.7%) were readmitted with HOS. The HOS group index surgery laparoscopy rates were lower compared with the control group within this subgroup as well (28.6% vs. 49.4%, respectively; P= 0.04).
There was a significant decrease in renal function among the entire cohort between the creation of the DLI and its reversal as reflected by the creatinine ratio (Table 2). The mean baseline creatinine prior to the index surgery was 0.82 mg/dL, compared with a mean creatinine of 0.96 mg/dL upon admission to the reversal surgery (P< 0.0001). The creatinine ratio correlated with the degree of renal function impairment and was significantly higher among the HOS group compared to the control group (1.36 vs. 1.16, respectively; P< 0.0001). Sixty patients of the entire cohort (19.5%) have presented for reversal surgery with impaired kidney functions (defined as creatinine levels > 1.2 mg/dL).
Readmissions for high output stoma
The median interval time between the creation of DLI to its reversal was 26 weeks (range, 10–88 weeks). The HOS group had a longer interval time compared to the control group (median of 36 weeks vs. 24 weeks, respectively) but this difference was not statistically significant.
During this interval time, 41 patients (13.3%) were readmitted to the hospital due to dehydration and HOS. Single readmission was recorded in 26 patients (63.4%), 2 readmission events in 6 patients (14.6%), 3 readmission events in 4 (9.8%), and the remaining 5 (12.2%) had more than 4 readmission events each. In total, there were 73 events of readmission (23.7%) to the hospital due to HOS. The median LOS for those readmissions was 4 days (range, 1–30 days).
Subgroup analysis of only the 204 patients who had the stoma created electively during a low anterior resection for rectal cancer showed similar results, with 48 events of HOS readmissions (23.5%). Nearly all patients (97.6%) presented with acute kidney injury on readmission with an average serum creatinine level of 2.62± 1.8 mg/dL compared to 1.02 mg/dL at baseline. Electrolyte abnormalities (hyponatremia/hypernatremia or hypokalemia/hyperkalemia) were common as well, with 75.6% sodium disturbances, and 53.7% potassium disturbances.
Risk factors for high output stoma
Multivariate analysis found high serum creatinine levels at index surgery, advanced ASA PS classification, and open approach and ileocolic resection at index surgery to be significantly associated with a risk for HOS.
Diabetes mellitus, congestive heart failure, and preoperative steroids were found to be associated with HOS on univariate analysis but not after multivariate analysis (Table 3). Adjuvant chemotherapy was not a risk factor for HOS.
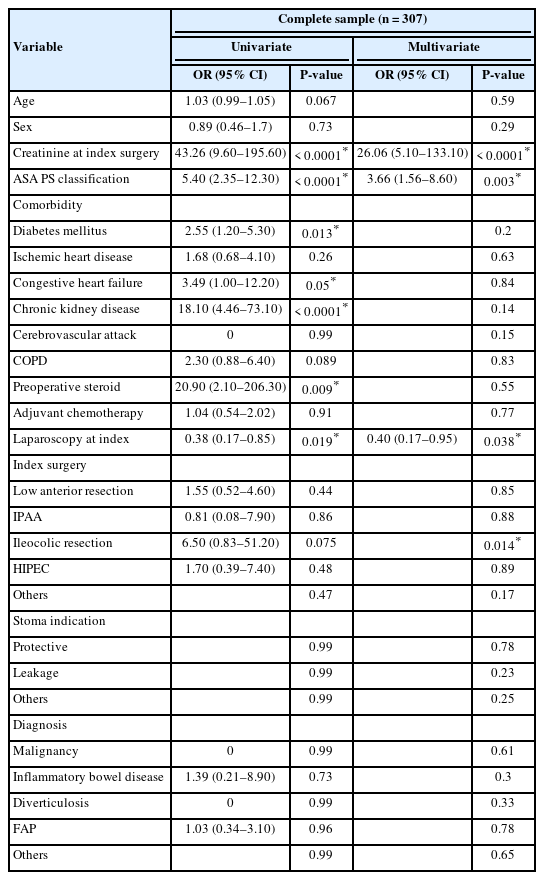
Univariate+multivariate association with high output stoma
DISCUSSION
Fluid and electrolytes abnormalities are the most frequent cause for hospital readmission following the formation of an ileostomy, with up to 20% readmission rates [13, 16, 17]. Those abnormalities are usually attributed to HOS in which increased loss of water and sodium in the fecal drainage leading to dehydration, hyponatremia, and hyperaldosteronism [17, 18].
In the present study which included 307 patients with DLI, 13.3% of the patients were readmitted for fluid and electrolytes imbalance, while the actual total readmission rate for dehydration (including all events) was 23.7%. Those rates are similar to previously reported literature. Hayden et al. [16] reported a 20% readmission rate for dehydration in a series of 154 patients with ileostomies (including both loop and end ileostomies). Those readmissions are usually severe with a significant acute kidney injury and significant LOS. This substantial readmission rate together with a non-negligible LOS during those readmissions creates an enormous burden on medical systems and medical staff, and of course, endangers the patients.
Upfront identification of risk factors for HOS could help health care providers in early therapeutic interventions to prevent or minimize HOS and the renal injury associated with it.
We found advanced ASA PS classification and impaired baseline kidney function as expressed by elevated creatinine levels to be significantly associated with readmission for HOS both in univariate and multivariate analysis. This is reasonable since patients with poor kidney function are more vulnerable to fluids and electrolytes loss and probably their adaption mechanisms that help most patients accommodate to the new ileostomy status are less effective.
Interestingly, we found that patients whose index surgery was done via laparoscopy were significantly less susceptible to readmission for HOS compared with patients who were operated through an open midline laparotomy. One possible explanation is that the open approach by itself is not a true risk factor for HOS but rather a surrogate for more complex patients such as patients who underwent CRS+HIPEC or more complex colorectal procedures. However, this theory is challenged by our subgroup analysis for just those who had the stoma done during an elective low anterior resection and which have shown similar results about those positive effects of laparoscopic surgery.
We found diabetes mellitus to be risk factor for HOS in a univariate analysis but not in a multivariate analysis. This is in correlation with a previous study by Takeda et al. [19] who also found diabetes to be a predictor of HOS. The autonomous nervous system impairment in diabetes decreases motor function of the bowel, which leads to abnormal proliferation of gas-forming bacteria primarily in the proximal small bowel [20, 21]. The gas increases the intestinal pressure, and this may increase the stoma output. Preventive protocols which include strict perioperative management of blood glucose levels could help in reducing the incidence of HOS.
Takeda et al. [19] also found total proctocolectomy to be a predictor of HOS. We haven’t found such a correlation. They speculate that total proctocolectomy prevents reabsorption of bile acids that are usually absorbed by the ileocecum, and that inhibits lipids absorption. The unabsorbed lipids are hydroxylated by intestinal bacteria, which triggers the secretion of fluids and electrolytes, and that may lead to HOS [22]. In addition, bile acid depletion might change the intestinal flora which in turn could increase intestinal drainage as well [22]. The authors suggested that bile acids supplementation in patients that have undergone total proctocolectomy might decrease their HOS [19].
Hayden et al. [16] found that the use of antidiarrheal such as loperamide, and neoadjuvant therapy for rectal cancer were associated with readmission for fluids and electrolytes abnormalities. The authors concluded that the use of antidiarrheal by itself is not a risk factor for readmission, but rather a marker for patients at risk for fluids and electrolytes abnormalities, and those patients should be strictly monitored at home. Antidiarrheal use was not part of the factors we evaluated in this current study. However, we did study the impact of adjuvant chemotherapy on the incidence of HOS and it was not a significant risk factor.
Patients who have been readmitted once with dehydration and HOS are at risk for recurrent readmissions for the same reason. A total of 37% of the patients presented with HOS in our cohort had multiple readmissions. Therefore, it is crucial to educate those patients prior to discharge regarding HOS and its management and prevention since they are at risk for recurrent episodes of HOS.
Besides acute episodes of dehydration and HOS among some of the patients with ileostomy as described, there is also a significant degree of renal impairment among all patients with ileostomy. In our overall cohort, the creatinine levels were significantly increased at the time of ileostomy reversal compared with the levels at the index surgery. This means that basically all patients with a DLI are at risk for renal injury, despite the fact that the ileostomy was created in the patient`s best interest. Similar findings were shown by Beck-Kaltenbach et al. [13]. They reviewed 107 patients with DLI and found a significant decrease in GFR between the creation of the stoma and its closure.
In concordance with previous literature we didn’t find an association between the time intervals from stoma construction to closure to HOS readmissions episodes. There is still controversy regarding the ideal time for ileostomy closure. Some authors advocate for early stoma closure since delayed closure was found to be associated with higher rates of stoma-related complications [23, 24]. However, since many rectal cancer patients are scheduled for adjuvant chemotherapy for a total of 6 months, the stoma closure is delayed until the completion of this treatment. Patients who present with HOS or those at risk for HOS should be considered for early closure of the stoma if the oncological status allows it or even prior to the initiation of adjuvant treatment.
Our study is limited by its retrospective nature. The study was conducted in a single medical center therefore the conclusions may be interpreted with caution. Our cohort wasn’t homogenous, although most of our patients were operated on for cancer, there were some patients who had different diagnoses such as diverticulitis or IBD. Still, we have confronted this cohort heterogenicity by subgroup analysis which showed similar results as described. Our data lacks information regarding daily stoma output, patient’s oral intake, and data regarding the use of antidiarrheal medications which was beyond the scope of this work but is important in forming strategies and protocols to prevent HOS readmissions.
In conclusion, DLI formation is associated with a substantial readmission rate for dehydration and HOS, and with a risk for renal impairment during the duration of the diversion. We identified advanced ASA PS classification, open surgery, and elevated baseline creatinine as predictors for HOS. The patients at risk should be identified prior to discharge to enable early prevention and intervention protocols including strict monitoring at home, and even at the time of primary surgery to consider whether a DLI is really necessary.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
None.
AUTHOR CONTRIBUTIONS
Conceptualization: DA, LS; Data curation: DH, ABY, LS; Formal analysis: all authors; Investigation: all authors; Methodology: all authors; Project administration: DA, LS; Resources: DZ, LS; Software: LS; Supervision: DA, LS; Validation: all authors; Visualization: all authors; Writing–original draft: all authors; Writing–review & editing: all authors. All authors read and approved the final manuscript.