Ileocolonic intussusception caused by epithelioid leiomyosarcoma of the ileum: a report of case and review of the literature
Article information

Abstract
Small intestinal malignant tumor accounts for about 3% of all malignant tumors in the gastrointestinal tract, among which 13% are leiomyosarcoma (LMS). In addition, epithelioid LMS is of very rare occurrence. As small intestinal malignant tumors are initially asymptomatic and nonspecific, diagnosis is often delayed, and this can lead to large tumor at the time of detection and lead to intussusception. We observed ileocolonic intussusception in an 80-year-old male patient who was admitted to the hospital with a complaint of abdominal pain and palpable mass on right lower quadrant. The laparoscopic ileocecectomy was performed by the emergency operation because of obstruction. The pathologic examination revealed that the epithelioid LMS developed in the terminal ileum was the leading point of intussusception. To the best of our knowledge, laparoscopic surgery for ileocolonic intussusception with epithelioid LMS has not yet been reported.
INTRODUCTION
Intussusception is known as the most common cause of intestinal obstruction in children under 2 years of age, and is the second most common cause of emergency surgery in children, after acute appendicitis [1]. However, about 5% of all intussusception occurs in adults [2]. Unlike pediatric cases, adult intussusception has a leading point or a specific cause in about 80% [3] and about 2/3 of them can be found in the small intestine. Most of these cases are caused by benign tumors such as small intestinal lipoma or an adenomatous polyp, and rarely caused by small intestinal malignant tumor in adults [2].
Small intestinal malignant tumors are of rare occurrence and constitute less than 3% of all gastrointestinal (GI) tract malignant tumors [4]. Histologically, small intestinal tumors are of different subtypes, with adenocarcinoma being the most frequent (47%) followed by carcinoid tumors (28%), leiomyosarcoma (13%), and lymphomas (12%) [5]. Most of them are asymptomatic or initial symptoms are nonspecific. Diagnosis of malignant tumors is often delayed, and it takes about 6 to 9 months to diagnose after symptoms appear, making early diagnosis a difficult task [6]. We report a case of ileocecal intussusception on abdominal computed tomography of an 80-year-old man with right lower abdominal pain. After surgical resection, ileal epithelioid leiomyosarcoma was diagnosed. To the best of our knowledge, this is the first report about a case of ileocolonic intussusception caused by epithelioid leiomyosarcoma of the ileum. This study was approved by the Institutional Review Board of Gyeongsang National University Hospital (GNUH 2019-01-024-001), and the informed consent was obtained.
CASE REPORT
An 80-year-old male patient visited the hospital with a complaint of abdominal pain on right lower quadrant which occurred 3 days ago. Ten months ago, he was diagnosed with non-small cell lung cancer and received radiation therapy. He was treated with a gamma knife 2 months ago for bleeding from brain metastases. Clinical examination demonstrated a tender and palpable mass in the right lower quadrant. He was hemodynamically stable. Detailed laboratory studies showed all results within normal limits, including complete peripheral blood cell counts and blood biochemistry. However, erythrocyte sedimentation rate was 69 mm/hr and C-reactive protein was 24.3 mg/L. About 5.5× 4.0-cm low-density mass in the terminal ileum and ileocolonic intussusception was observed on the computed tomography scan (Fig. 1).

Abdominal computed tomography of abdomen and pelvis with contrast. An ileocolic intussusception is present (arrows) with the terminal ileum telescoping into the ascending colon. (A) Axial view, (B) coronal view.
He underwent an emergency operation using a laparoscopic technique on the same day and ileocolonic type of intussusception was confirmed based on the examination of the abdominal cavity with a camera (Fig. 2). Laparoscopic-assisted ileocecal resection was performed for the treatment of lesions. In the excised colonic specimen, around 4× 3 cm of ulcerofungating mass was observed (Fig. 3). Microscopic examination revealed the tumor as epithelioid leiomyosarcoma with extension to subserosa and 40 mitoses per 10 high-power fields (Fig. 4). Immunohistochemistry of the tumor cells revealed the presence of vimentin and smooth muscle actin (SMA). Among the other markers, CD117 showed a weak positive, but desmin, CD117, discovered on GI stromal tumor 1 (DOG-1), S-100, human melanoma black (HMB)-45, and calponin were negative (Fig. 5). In addition, CK7, CK20, epithelial membrane antigen (EMA), and leukocyte common antigen (LCA) were also negative and not included in the figure. The proximal and distal resection margins measured 10.5 and 15 cm, respectively. No metastasis was found in any of the 14 removed lymph nodes. He was discharged without complications after surgery but died 3 months after surgery from a worsening non-small cell lung cancer.
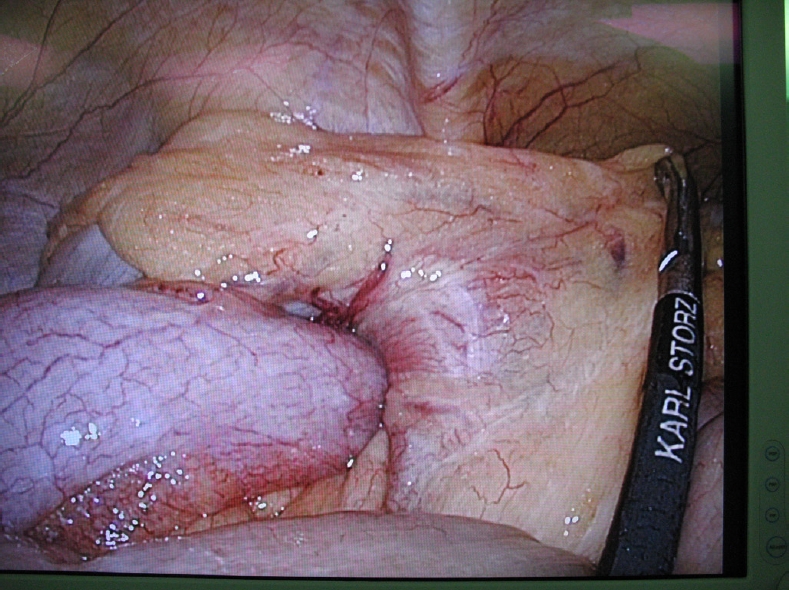
Intussusception of the ileum into the cecum is seen on the laparoscopic screen.

Gross finding of a 3.5×2.5-cm sized tumor in terminal ileum.

Microscopic findings of epithelioid leiomyosarcoma. (A) The tumor shows lobular growth pattern and extension proper muscle and subserosa (H&E, ×20). (B) The tumor cells have eccentric round-to-ovoid vesicular nuclei with inconspicuous nucleoli and abundant vacuolar to lightly eosinophilic cytoplasm. Numerous mitotic figures (arrows) are found up to 40 per 10 high-power fields (H&E, ×400).

Immunohistochemistry of epithelioid leiomyosarcoma. The tumor cells express (A) vimentin and (B) smooth muscle actin. The other markers, (C) desmin, (D) CD117, (E) DOG-1, (F) S-100, (G) HMB-45, and (H) calponin are weak positive (only for CD117) or negative (×200). DOG-1, discovered on gastrointestinal stromal tumor 1; HMB-45, human melanoma black 45.
DISCUSSION
Small intestinal malignant tumors are rare and comprise less than 3% of all primary GI neoplasms [4]. There are several conditions that increase the risk of development of small intestinal malignancies, including inflammatory bowel diseases such as Crohn disease, polyposis syndrome, and hereditary nonpolyposis colorectal cancer [7].
Leiomyosarcoma arising in the GI tract accounts for 1% to 2% of GI malignancies and the distribution of the lesions is 50% in the stomach, 30% in the small intestine, 15% in the colon, and 5% in the esophagus [8]. Leiomyosarcoma of the small intestine occurs in the order of the jejunum, the ileum, and the duodenum [9].
Leiomyosarcoma is histologically composed of spindle cells with moderate or more differentiation but epithelial cells or a mixture of these 2 types of cells may appear. Epithelioid leiomyosarcoma is characterized by round to polygonal cells with abundant eosinophilic or clear cytoplasm. In the present case, eccentric round-to-ovoid vesicular nuclei with inconspicuous nucleoli were detected in the pathologic examination [10]. Additional immunohistochemistry tests were used to confirm the diagnosis.
Differential diagnosis which shows similar histologic finding with this case includes epithelioid leiomyoma (positive for SMA and usually negative for desmin), epithelioid GI stromal tumor (positive for CD117 and DOG-1), perivascular epithelioid cell tumor (positive for SMA, S-100, and HMB-45), clear cell sarcoma (positive for S-100 and HMB-45), and malignant glomus tumor (positive for SMA and calponin). Although not shown in the figure, additionally, CK7, CK20, EMA, and LCA were negative. Considering the results of immunohistochemical stains, the diagnosis was consistent with epithelioid leiomyosarcoma.
The clinical features of small intestinal malignant tumors are unfortunately very nonspecific. The patient may have abdominal pain, nausea and/or distension. In the early stages, these symptoms can be misdiagnosed as other benign diseases such as functional GI impairment, which can delay the diagnosis [11]. Because the clinical symptoms are nonspecific, a high index of suspicion is needed to diagnose small intestinal malignant tumors. In later stages, iron deficiency anemia or GI bleeding may be accompanied, but in most of the cases, the amount of hemorrhage is low and the diagnosis is made based on fecal occult blood test rather than by hematochezia [11, 12]. Unfortunately, the presence of obvious symptoms reveals local invasion or metastasis, and prognosis may be worse [13].
The only effective treatment of leiomyosarcoma in the small intestine is surgical resection, which is known to require extensive resection including the mesentery, and radiation therapy for leiomyosarcoma of the small intestine has yet to provide clear evidence. It is also known that chemotherapy has a very low response. The clinical differences between leiomyosarcoma and epithelioid leiomyosarcoma in the conventional small intestine are very rare in the latter case, so they are not clearly known.
In the present case, the patient presented with right lower quadrant abdominal pain which led to the detection of a tumor in the terminal ileum. An ileocecectomy was performed using a laparoscope based on the diagnosis of ileocolonic type intussusception. Pathological examination of the small intestine after surgery revealed the presence of epithelial leiomyosarcoma. In the past, no cases of laparoscopic ileocecectomy with ileocolonic intussusception due to small intestinal epithelial leiomyosarcoma have been reported. However, the PubMed database search presented a case of segmental laparoscopic resection of the small intestine due to leiomyosarcoma described by Hamm et al. in 2013 [14]. One case of laparoscopic resection with ileocolonic intussusception caused by ileal leiomyosarcoma described by Guzel et al. in 2016 [7] was evident, although it was not a case of epithelioid leiomyosarcoma.
In conclusion, leiomyosarcoma of the ileum is rare and the symptoms are nonspecific, making it difficult to identify at the first diagnosis. However, in the present case, we experienced a rare case of epithelioid leiomyosarcoma of the ileum, which was found to be the leading point for ileocolonic intussusception.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING
This study was supported by grants of the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Plan ning, Republic of Korea (No. NRF-NRF-2018R1D1A1B07045469).