Short-term and Medium-term Outcomes of Low Midline and Low Transverse Incisions in Laparoscopic Rectal Cancer Surgery
Article information

Abstract
Purpose
Limited data exist on the use of low midline and transverse incisions for specimen extraction or stoma sites in laparoscopic rectal cancer surgery (LRCS). We compared the short-term and medium-term outcomes of these incisions and assessed whether wound complications in specimen extraction sites (SES) are increased by specimen extraction through the stoma site (SESS) in LRCS.
Methods
From March 2010 to December 2017, 189 patients who underwent LRCS and specimen extraction through low abdominal incisions were divided into 2 groups: midline (n = 102) and transverse (n = 87), and perioperative outcomes were compared.
Results
The midline group showed a higher frequency of temporary stoma formation (P = 0.001) and splenic flexure mobilization (P < 0.001) than the transverse group. The overall incisional hernia and wound infection rates in the SES were 21.6% and 25.5%, respectively, in the midline group and 26.4% and 17.2%, respectively, in the transverse group (P = 0.494 and P = 0.232, respectively). In patients who underwent SESS, the incisional hernia and wound infection rates of SES after stoma closure were 39.1% and 43.5%, respectively, in the midline group, and 35.5% and 22.6%, respectively, in the transverse group (P = 0.840 and P = 0.035, respectively).
Conclusion
In terms of incisional hernia and wound infection at the SES, a low midline incision may be used as a low transverse incision in patients without temporary stoma in LRCS. However, considering the high wound complication rates after stoma closure in patients with SESS in this study, SESS should be performed with caution in LRCS.
INTRODUCTION
A mini-laparotomy for specimen extraction following laparoscopic colorectal surgery is usually performed through a transverse or midline incision of the abdomen [1, 2]. However, potential complications, such as incisional hernia, wound infection, and tumor seeding to the wound, may occur [2-4]. Although some studies have reported that low transverse and umbilical incisions as specimen extraction sites (SES) have a similar incisional hernia and wound infection rates after laparoscopic colorectal surgery [5-7], a low transverse incision is recommended because the incisional hernia rate is lower than in midline incision [1-3, 8-10].
Laparoscopic rectal cancer surgery (LRCS) has been advantageous in postoperative recovery, and with oncologic results similar to those of open surgery in large randomized studies [11, 12]. Thus, the application of this procedure is increasing [13]. Specimen extraction following LRCS is possible through the anus [14- 16], but in most cases, it is achieved through the low transverse abdomen, midline abdomen, or potential stoma site [1, 5, 17-19]. Some studies [17-19] have also attempted specimen extraction through a stoma site (SESS) to minimize additional mini-laparotomy for a temporary diverting stoma in LRCS. Recent studies [20, 21] have reported the feasibility of SESS utilizing umbilicus in LRCS. Based on these studies [17-21], a low midline incision with benefits in respiratory function, pain intensity [22], and minimizing additional mini-laparotomy for a temporary diverting stoma may also be considered for the SES during LRCS. Previous reports [17-19] about specimen extraction or stoma sites in LRCS focus only on the short-term results of a low transverse incision, and thus are lacking data on low midline incisions or medium-term results, such as the incidence of incisional hernia and wound infection, at the SES after stoma closure in patients who undergo SESS.
Thus, the aim of this study was to compare the results of low midline and low transverse incisions and to evaluate the usefulness of a low midline incision in LRCS. Furthermore, we assessed whether the wound complications at SES are increased by SESS in LRCS.
METHODS
The Institutional Review Board of Inje University Haeundae Paik Hospital approved the study protocol (No. HPIRB 2019-07-025-002) and written informed consent was obtained from all patients before surgery.
A total of 330 consecutive rectal cancer patients who underwent laparoscopic surgery between March 2010 and December 2017 were identified from the colorectal cancer databases recorded in a prospective manner at the authors’ institutions. Of the 330 patients, the following 141 patients were excluded: (1) specimen extracted through upper midline, transumbilical, and Pfannenstiel incision (n= 77); (2) patients who did not undergo mini-laparotomy incision due to totally laparoscopic rectal resection (n= 18); (3) patients without temporary stoma closure (n= 18); (4) patients who were not followed up immediately after surgery (n= 14); (5) patients who underwent abdominoperineal resection or Hartmann type resection (n= 10); and (6) conversion to open surgery (n = 4). A total of 189 patients excluding the above-mentioned were enrolled in this study. A low midline incision was preferentially performed in patients with a relatively short distance from the symphysis pubis to the umbilicus or a previous low midline incision. The patients were divided into 102 who underwent LRCS through a low midline incision (midline group) and 87 who underwent LRCS through a right or left low transverse incision (transverse group) as the SES. The clinical characteristics of the patients and perioperative outcomes were analyzed retrospectively.
Surgery was performed by a single colorectal surgeon and the first mini-laparotomy was performed according to tumor size in a similar manner to single port laparoscopic surgery. The wound was applied with an Alexis wound protector (Applied Medical, Rancho Santa Margarita, CA, USA). One 5-mm and one 12-mm trocar were placed in 2 surgical glove fingers (‘glove port’) and attached to the wound protector (Fig. 1). Following pneumoperitoneum, a 5-mm laparoscopic camera port was inserted in the umbilicus and an additional port was placed in the right or left abdomen according to the abdominal incision (Fig. 2). The brief operative procedure was as follows: the inferior mesenteric artery was mostly high ligated, and the left colon was separated from the left retroperitoneum. The rectum was mobilized down to the pelvic floor muscle level or below. After washing the rectum below the tumor with a povidone solution, the rectum was cut through a 12-mm port located in the glove port. Following specimen extraction, the anastomosis of the intestinal tract was performed using a circular stapler and a reinforcement suture at the anastomotic site was performed intracorporeally. When anastomosis using a circular stapler was difficult, hand-sewn coloanal anastomosis was performed. Temporary diverting stoma was created at the discretion of the surgeon in cases of very low anastomosis (anastomosis within 2 to 3 cm of the anal verge), difficult pelvic dissection, positive air leak test, poor bowel preparation, or the poor general condition of patients. A temporary stoma was created via a low midline incision with SESS or a separate right lower transverse incision with no SESS in the midline group, and a right (left) lower transverse incision with SESS or a separate right (left) upper transverse incisions in the transverse group. When a difference in size exists between the stoma and the mini-laparotomy incision, the SES was adjusted to the size of the stoma by peristomal suture.
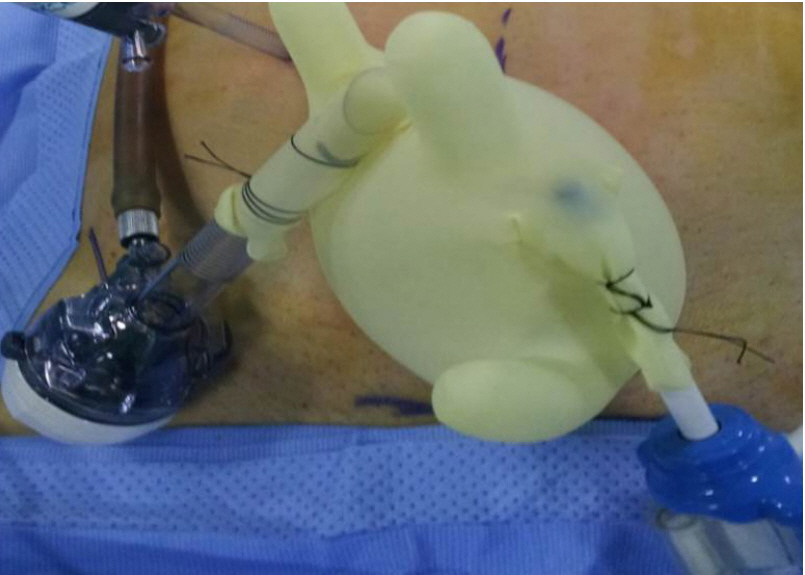
Home-made “glove port”. One 5-mm and one 12-mm trocar were placed in 2 surgical glove fingers and attached to the wound protector.

(A) Port placement for patients who underwent laparoscopic rectal cancer surgery (LRCS) using a low midline incision. (B) Port placement for patients who underwent LRCS using a low transverse incision.
On the day before surgery, oral antibiotics (metronidazole and tetracycline), and sodium picosulfate or bisacodyl were used for bowel preparation. Intravenous patient-controlled anesthesia with fentanyl was used for postoperative pain management. Most abdominal incisions were closed by the operating surgeon with a polyglactin using an interrupted method. Abdominal closures after stoma closure were performed using a single layer interrupted closure technique of the fascia and peritoneum with polyglactin in both groups. Until 2011, conventional primary linear sutures were used for skin closure; however, since 2012, a single-layer subcutaneous suture using a semi-closed method was performed with gauze dressing in both groups. In most patients who underwent stoma closure, a wound drainage tube was not inserted.
The amount of blood loss during surgery was calculated by subtracting the volume of instilled fluids from the volume of aspirated fluids. Postoperative complications occurring within 30 days after surgery, except for incisional hernia, were included and graded using the Clavien-Dindo classification. An incisional hernia was defined as an abdominal wall gap in the SES, trocar site, and additional stoma site by using abdominal computed tomography. It was evaluated after stoma closure in patients with a temporary stoma. Diagnosis of wound infection was considered positive when any of the following events occurred: purulent discharge; positive wound culture; clinical symptoms or signs, such as pain, erythema, and edema; and wound opening by the surgeon for wound debridement or wound drainage. In the event of wound infection, the wound was managed by wound opening and wound debridement, if necessary, at the bedside during hospitalization or the outpatient clinic, and allowed to heal by a second intention. Wound infection was graded according to classification by Dindo et al. [23]. Grade I infection was defined as a wound infection treated by a wound opening. Grade II infection was defined as a wound infection requiring antibiotic treatment because of additional phlegmonous infection.
Statistics
Statistical analysis was performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were analyzed using a chi-square or Fisher exact test, and continuous variables were tested by independent t-test. A P-value less than 0.05 was considered statistically significant.
RESULTS
Comparison of clinical variables in both groups of patients
The mean values of the body mass index were 23.7 and 24.2 (P= 0.344), with a mean age of 64.3 and 64.9 years (P= 0.733) in the midline and transverse groups, respectively. The incidence of tumors located below the anterior peritoneal reflection was 52.0%, and the abdominal operation history was 24.5% in the midline group. No statistically significant difference was found in tumor size, preoperative radiotherapy frequency, and stage distribution between the 2 groups (Table 1).
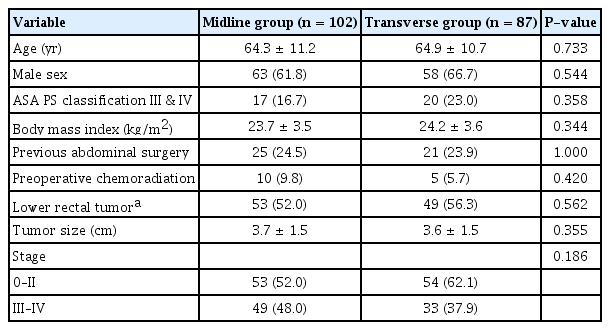
Clinicopathologic features of patients classified according to the mini-laparotomy incision site
Short-term outcomes following surgery
The mean length of the mini-laparotomy was 4.5 cm in the midline group, but it was not significantly different from 4.2 cm in the transverse group (P= 0.874). The mean values of operation time and blood loss were 284.3 minutes and 156.0 mL, respectively, and no statistically significant difference was found between the 2 groups. Moreover, no significant difference was noted in the incidence of circumferential resection margin involvement and adequate distal resection margin in the midline and transverse groups (P= 0.548, P= 0.154). The incidence of additional abdominal incisions for the temporary stoma was 8.0% in the midline group and 3.1% in the transverse group (P= 0.231). There was a lower rate of temporary stoma formation (P= 0.001) and a higher rate of splenic flexure mobilization (P < 0.001) in the midline group than in the transverse group (Table 2).
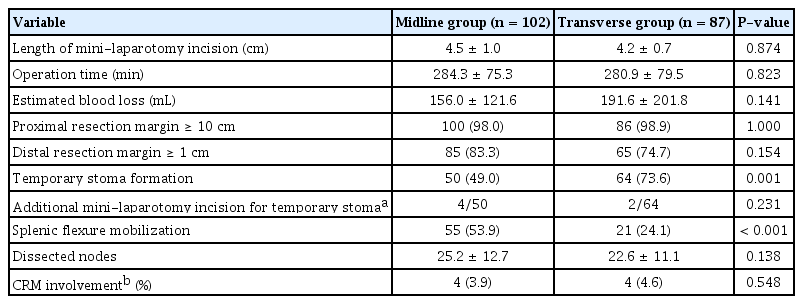
Comparison of operative results of patients classified according to the mini-laparotomy incision site
Postoperative recovery variables, such as first gas or stool passage, postoperative pain score, and length of hospital stay, were similar in the midline and the transverse groups (Table 3).

Postoperative recovery outcomes of patients classified according to the mini-laparotomy incision site
Postoperative complications
Among the Clavien-Dindo complications classified as mild grade I or II, postoperative voiding dysfunction was the most common in both groups (12.7% in the midline group and 11.5% in the transverse group). Purulent or turbid discharge was released from the abdominal drainage tube in 9 patients in the midline and transverse groups. Severe complications of Clavien-Dindo grade III or higher occurred in 3 patients (2.9%) in the midline group and in 3 patients (3.4%) in the transverse group (P= 0.827). The incidence of overall complications within 30 days after surgery was similar in both groups (P= 0.780) (Table 4).

Clavien-Dindo classification of early complications of patients classified according to the mini-laparotomy incision site
Wound complications in SES
The overall incisional hernia rate was 21.6% in the midline group and 26.4% in the transverse incision group (P= 0.494), with a median follow-up period of 31 months (range, 4 to 90 months). No incisional hernia or wound infection occurred except in the SES. In patients who did not undergo temporary stoma, the incisional hernia rate of the SES was 7.1% in the midline group and 4.0% in the transverse group (P= 0.507). The wound infection rate after stoma closure in patients with SESS was 43.5% in the midline group and 22.6% in the transverse group (P = 0.035). Wound complications in relation to whether the specimens were extracted through the stoma site were compared. In patients whose incisions were only used for specimen extraction (n= 81) the incisional hernia and wound infection rates of the SES were 6.2% and 8.6%, respectively, and in patients who underwent SESS (n= 108) the incisional hernia and wound infection rates of the SES after stoma closure were 37.0% and 31.5%, respectively (both P < 0.001). However, the rate of the grade II wound infection in the midline group (n= 46) was comparable to that in the transverse group (n= 62) in the patients who underwent SESS (P= 0.643) (Table 5).
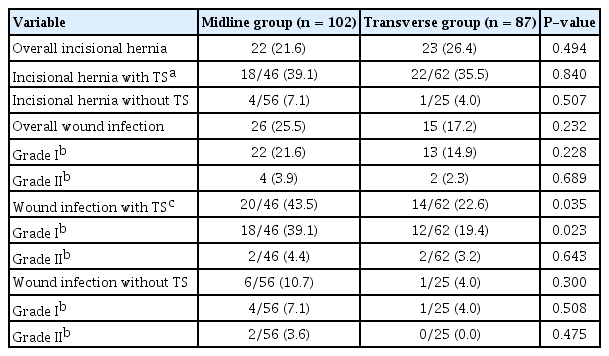
Wound complications in the specimen extraction site
DISCUSSION
While a low transverse incision was reported to be the preferred extraction site during LRCS [17-19], the use of a low midline incision as an SES has rarely been reported in LRCS. In this study, the incisional hernia rate in the SES following LRCS was not significantly different between the low midline and low transverse incisions. In addition, among the 81 patients who did not undergo SESS, incisional hernia rates of 7.1% and 4.0% at the SES in the low midline incision and low transverse incision groups, respectively, were comparable. There was no significant increase in the wound infection rate in the low midline incision group following LRCS; however, in the 108 patients who underwent SESS, after stoma closure, the wound infection rate with a low midline incision was approximately 44% and significantly higher than that with the low transverse incision of approximately 23%.
A temporary diverting stoma was performed in 35% to 80% of patients who underwent LRCS [11, 24], and the possibility of additional abdominal incision for temporary stoma is high in addition to the incision for specimen extraction. Previous studies [17-21] have reported that the SESS is performed through the right (left) low abdomen or umbilical site to maintain the advantages of minimally invasive surgery by reducing the need for an additional minilaparotomy for temporary stoma during LRCS. The present study results also showed that 108 of 114 patients (94.7%) who required temporary stoma had stoma formation through an SES, and the incidence of the requirement for an additional mini-laparotomy for temporary stoma was comparable between the 2 groups. This finding suggested that a low midline incision in LRCS may also have the advantage of reducing the requirement for an additional mini-laparotomy for temporary stoma, same as that for a low transverse incision. In addition, consistent with the study of Wang et al. [17], who reported no increase in the prevalence of peristomal morbidity in patients who underwent SESS, no serious complications of peristomal wound occurred in our midline group.
We defined incisional hernia as an abdominal wall gap regardless of clinical symptoms on computed tomography. Based on computed tomographic findings, the incidence of overall incisional hernia of the SES in the present study was 21.6% in the midline group and 26.4% in the transverse group. Although the incisional hernia rate in the SES in our study was higher than that reported in a previous study [25] of approximately 10% in low midline or low transverse incision, it is presumed that in 50% or more of patients the specimen was extracted via the temporary stoma site, which may be a risk factor of incisional hernia after temporary stoma closure [25, 26]. However, the comparable incisional hernia rates after LRCS between the 2 groups in our study were somewhat different from those reported in a systematic review [10]. The systematic review reported that the incisional hernia rate in the midline incision was 3 times higher than that in transverse incision. Because abdominal wound closure was mostly performed by the attending surgeon in our institution, the similar incisional hernia rates in both groups in our study may be explained by the study of Navaratnam et al. [27], who reported the incidence of incisional hernia is minimized even in the midline incision using the standardized technique. However, some studies [9, 28] denoted that midline incision has a higher incisional hernia rate even when using the standardized technique for wound closure during laparoscopic colectomy.
Benlice et al. [25] reported that the incisional hernia rate was significantly increased by 28 times in SESS. In concordance with this study, our results demonstrated an incisional hernia rate of 37% in patients where mini-laparotomy is used for synchronous temporary stoma formation compared with that of 6% in the patients where mini-laparotomy is only used for specimen extraction (P< 0.001). However, when the SES is not used for temporary stoma, our incisional hernia rates of the SES were 7.1% and 4.0% in the low midline and low transverse incisions, respectively (P= 0.507), and these results are similar to those of previous studies reporting an incisional hernia rate of approximately 10% in low midline incision and approximately 4% in low transverse incision following LRCS [9, 25, 28]. Based on these results, with respect to incisional hernia, low midline incision, if not used for temporary stoma formation, may be used as the SES in low transverse incision during LRCS.
In this study, the overall wound infection rate in the SES was not different statistically in 25.5% of the midline incision group and 17.2% of the transverse group (P= 0.232). However, in our 108 patients who underwent SESS, the wound infection rate after stoma closure in the SES was significantly higher in the midline group (43.5%) than in the transverse group (22.6%) (P= 0.035). Previous reports [8, 29] mention that the midline incision has the potential for impaired blood supply to the wound site during wound healing. In this study, it was postulated that wound infection was a higher rate in low midline incision than in low transverse incision in patients with SESS by the hypothesis that impaired blood supply to the low midline wound site combined with wound contamination during stoma closure may increase the likelihood of wound infection. In contrast to a recent meta-analysis [30], in which the wound infection rate was less than 10% following stoma closure in patients with rectal cancer, the wound infection rate of 31.5% after stoma closure in our 108 patients who underwent SESS seemed to be quite high. However, the wound infection rate after stoma closure in patients who underwent SESS in this study was interpreted on considering that the wound infection rate after stoma closure can reach 36% and may be higher than the usual rate reported in previous literature [31]. Another factor to consider about this high wound infection rate is an increased susceptibility to the formation of dead space due to myofascial dissection during wound closure, which may lead to an increased accumulation of exudate. Therefore, we attempted to minimize the accumulation of wound fluid and dead space formation by wound drainage and 2-layer subcutaneous suture during stoma closure in cases of SESS.
The authors’ surgical technique is somewhat different from the conventional 5-port laparoscopic surgery in that it is a modified 4-port technique in which a mini-laparotomy is first carried out. Although the port location of the transverse group was similar to that of conventional LRCS, the main procedure for dissection and transection of the rectum in the midline group was performed through the glove port located in the low midline abdomen. Our study showed that in a comparison of surgical technique related outcomes, the midline group was significantly superior to the transverse group in the frequency of temporary stoma formation and splenic flexure mobilization. Although disagreement exists as to which port to use for major surgical manipulation in LRCS [32], our findings suggest that the use of a working port located in the low midline abdomen has a positive effect on the surgical outcome.
This study has several limitations. First, although no significant difference was found between the clinical characteristics of the 2 groups, a possibility of bias exists in patient selection due to the retrospective study design. Second, because most specimens were extracted through the midline abdomen or right (left) low abdomen at our institution, this study did not include data on Pfannenstiel incisions with advantages in terms of wound complications [8, 33]. Third, this study did not include data on medical comorbidities, such as diabetes mellitus and obstructive lung disease that could affect wound complications after LRCS due to the limitations of the retrospective study. Despite these limitations, to the best of our knowledge, this is the first study to report a low midline incision as an SES in LRCS.
In conclusion, in relation to incisional hernia and wound infection at the SES, a low midline incision may be used as a low transverse incision in patients without temporary stoma in LRCS. However, considering the high rates of incisional hernia and wound infection after stoma closure in patients who underwent SESS through low midline or low transverse incisions in this study, SESS should be performed with caution in LRCS.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.