INTRODUCTION
Fecaliths and fecomucoliths can form in rectal stumps post-HartmannŌĆÖs procedure and other procedures such as coloneovaginoplasty. They are formed from retained stool and/or mucus in the bowel lumen which hardens over time. They can cause significant symptoms and when large and present for some time, they can be very difficult to treat. We describe a method that can be used when other methods such as enemas and removal of fecomucolith under anesthetic fails. An effective endoscopic method of obliteration and removal in this setting has not been published. However, a similar technique has previously been described for the removal of a fecalith at the appendiceal orifice via colonoscopy [1, 2]. Our endoscopic method is useful where other techniques such as removal with a pair of forceps under anesthesia or serial enemas have failed. Informed consent for publication has been obtained from the patient and this article has been written in line with institutional ethical guidelines.
TECHNIQUE
We report the use of a multi-method approach to this problem, which is particularly useful where other methods such as self-administering enemas or an examination under anesthetic and removal of fecalith fails due to stenosis at the anastomosis.
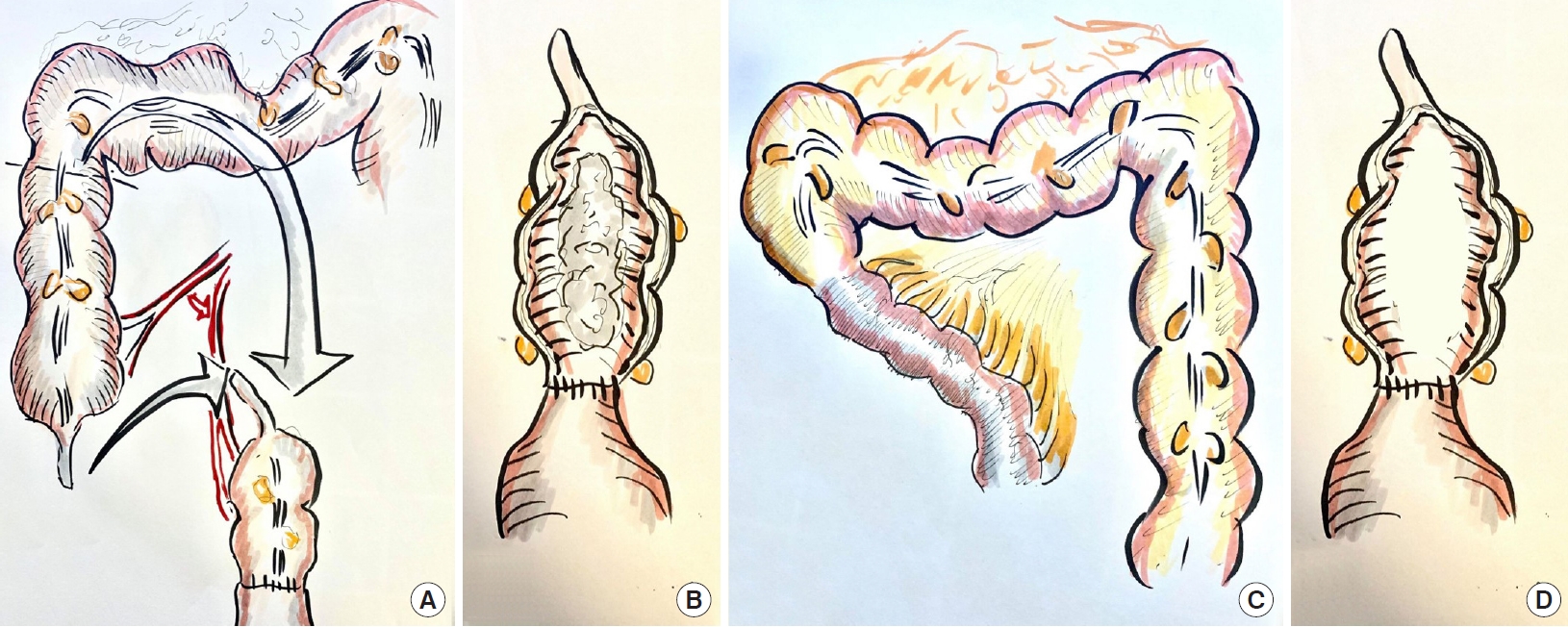
A 57-year-old male to female sex reassignment patient presented with offensive smelling discharge from a neovagina. This had caused significant distress and affected her personal and sexual relationships. The patient had previously undergone surgery 18 years prior where the penis skin was inverted to create a vaginal cavity. She then subsequently had a coloneovaginoplasty to increase the vaginal depth (Fig. 1). The patient was not performing the required daily neovaginal dilatation to prevent stenosis. She had delayed seeking medical treatment due to concern about stigma by wider community and from the medical profession despite the considerable effect of the odor and discharge on her self-esteem and relationships.
The cause for the presenting complaint was a large fecomucolith that had formed above the coloneovaginal anastomosis which was stenotic (Fig. 1). Other more traditional methods were initially used. The fecomucolith was unable to be grasped with Rampleys forceps under anesthesia and this only caused advancement of the fecomucolith to an inaccessible point. Further, stenosis of the anastomosis made passing instruments difficult. Enemas into the neovaginal cavity were also ineffective in removing the fecomucolith.
Therefore, a novel endoscopic method was developed which can be used where other methods such as removal under anesthetic and enemas have failed as in this case. The same technique has also been used by our group for an elderly patient with a fecalith within a rectal stump following a Hartmann procedure.
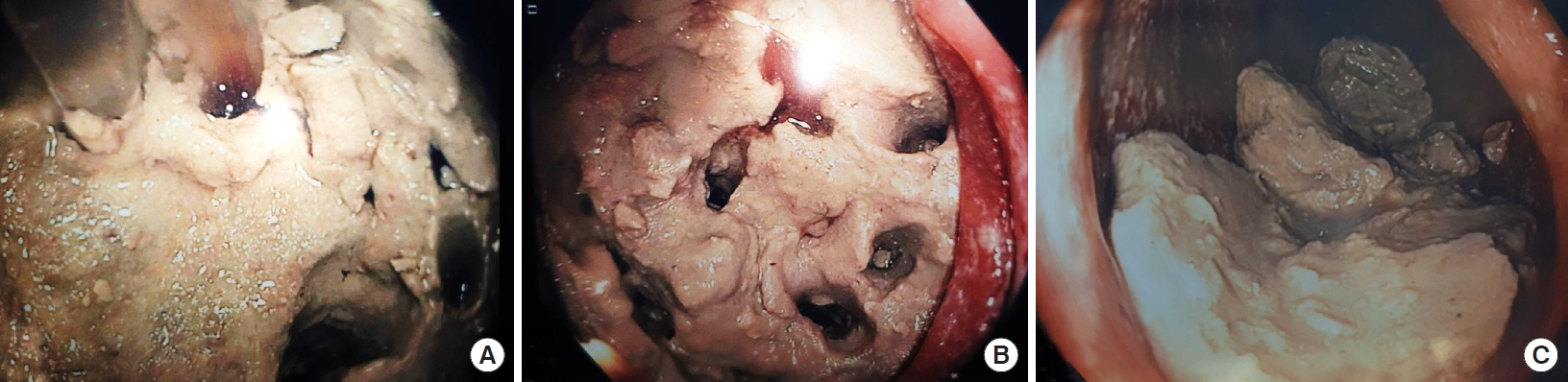
A colonoscope was passed to the point of the fecomucolith. Several techniques were used to break down and remove the fecomucolith. Firstly, the Interject Clear 23 gage injection needle catheter and saline injector gun (Boston Scientific, Marlborough, MA, USA) are used to hydrodissect holes into the fecomucolith (Fig. 2). This is done by injection in the same area with a high-pressure saline push. Multiple holes can be formed in the fecalith with this method. Then, large biopsy forceps are used to break down the fecalith by inserting the jaws closed into the holes and opening the jaws to fracture it. A large polypectomy snare (Captivator Extra Large Rounded Stiff braided 33-mm Polypectomy Snare; Boston Scientific) is used to break the fecalith into smaller pieces and shave softer segments of the fecalith off (Fig. 2). Finally, a retrieval net is used to retrieve the smaller pieces. Finally, a flushing pump and suction action are used to suction larger fragments onto the end of the scope to facilitate removal.
DISCUSSION
The fecalith was able to be successfully removed without any complications in this patient and the presenting symptoms resolved. The same result was achieved in the elderly patient who presented with a fecalith within the rectal stump after a Hartmann procedure. The risk of perforation of the colonic conduit is very low with this technique.
We recommend performing this procedure under general anesthetic in the lithotomy position. The surgeon should allow at least 2 to 3 hours for the case and it is not suitable for a routine endoscopy list. Our tips for this procedure include keeping the pouch well-inflated with air and irrigation fluid and pressing the fecalith into the apex of the conduit to prevent it from slipping away.
This technique is an effective and novel method for endoscopic removal of a fecalith or fecomucolith when removal under anesthetic and enemas have failed. Using a stepwise approach with multiple methods of dissection, this troublesome problem can be solved with readily available endoscopic devices.