Long, Pedunculated, Large Hyperplastic Polyp of the Terminal Ileum Protruding Through the Ileocecal Valve: A Case Report
Article information

Abstract
Small-bowel tumors, both benign and malignant, are rare lesions that clinicians often do not encounter, accounting for less than 2% of gastrointestinal malignancies. Usually, benign small-bowel tumors, including polyps, are asymptomatic. The diagnosis of small-bowel tumors is difficult because of an often-delayed presentation and nonspecific signs and symptoms. We report an incidentally detected case of a long, pedunculated, large polyp of the terminal ileum, which protruded through the ileocecal valve into the cecum that was removed by colonoscopy in a 41-year-old male with intermittent right-sided lower-abdominal pain. The polyp was resected through snare polypectomy without complications. The histopathology of the resected polyp was confirmed as an ileal hyperplastic polyp. Two years later, there was no recurrence observed via postpolypectomy surveillance colonoscopy.
INTRODUCTION
Small-bowel tumors, including both benign and malignant tumors, are lesions that clinicians often do not encounter. Smallbowel tumors are very rare, accounting for less than 2% of gastrointestinal malignancies [1]. Usually, benign small-bowel tumors, including polyps, are asymptomatic. Further, delayed presentation and nonspecific symptoms or signs can make the diagnosis of small-bowel tumors difficult [2]. However, sometimes, the tumors can cause small-bowel obstruction via the development of intussusceptions [3]. We describe an incidentally diagnosed case of a long, pedunculated, and large ileal hyperplastic polyp that was removed via colonoscopy in a 41-year-old male with intermittent right-sided lower-abdominal pain.
CASE REPORT
This study was approved by the electronic Institutional Review Board of the Korea National Institute for Bioethics Policy (P01-201809-21-001) and the need for informed consent was waived.
A 41-year-old male visited our clinic with intermittent right-sided lower-abdominal pain without diarrhea, fever, weight loss, or other general symptoms. His past medical history and family history were unremarkable. His laboratory blood test results including white blood cell count and hemoglobin, platelet, alanine aminotransferase, and aspartate transaminase levels were within normal limits. A viral marker test for hepatitis B and a serologic investigation for an immunocompromised state (i.e., human immunodeficiency virus antibody) yielded negative results. The rapid plasma reagin test for syphilis was nonreactive.
At this point, he underwent a colonoscopy, where 2 small sessile polyps of the sigmoid colon and a long, pedunculated polyp measuring about 2 cm with surface erosion of the terminal ileum protruding through the ileocecal valves into the cecum (Fig. 1A, B) were detected. After injection of an indigo carmine-epinephrine mixture at the base of the pedunculated ileal polyp, snare polypectomy was performed without complications (Fig. 1C). The prophylactic placement of one hemoclip to prevent delayed postpolypectomy bleeding was applied at the base of the resected ileal polyp (Fig. 1D). Subsequent histopathological examination of the resected ileal polyp revealed the proliferation of multiple glands and dilated glands without dysplasia with inflammatory cell infiltration in the stroma (Fig. 2). These findings were consistent with hyperplastic polyp. The postpolypectomy course was uneventful and the patient was discharged the next day. No recurrence was observed via postpolypectomy surveillance colonoscopy after 2 years (Fig. 3).
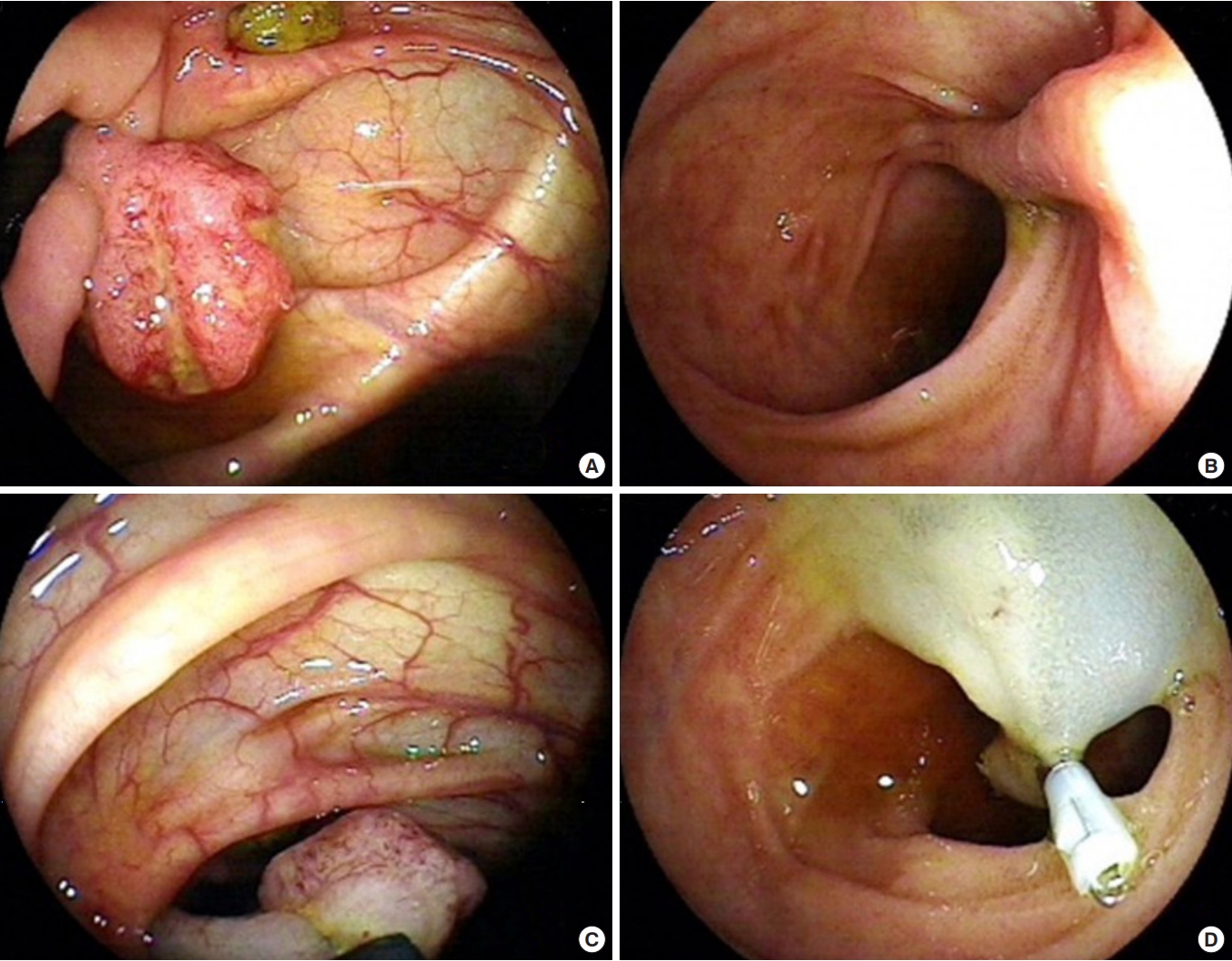
(A, B) A large, pedunculated ileal polyp with erosion was detected in the cecum during colonoscopy. (C, D) Snare polypectomy was performed after the injection of an indigo carmine-epinephrine mixture and a hemoclip was placed at the polyp base.
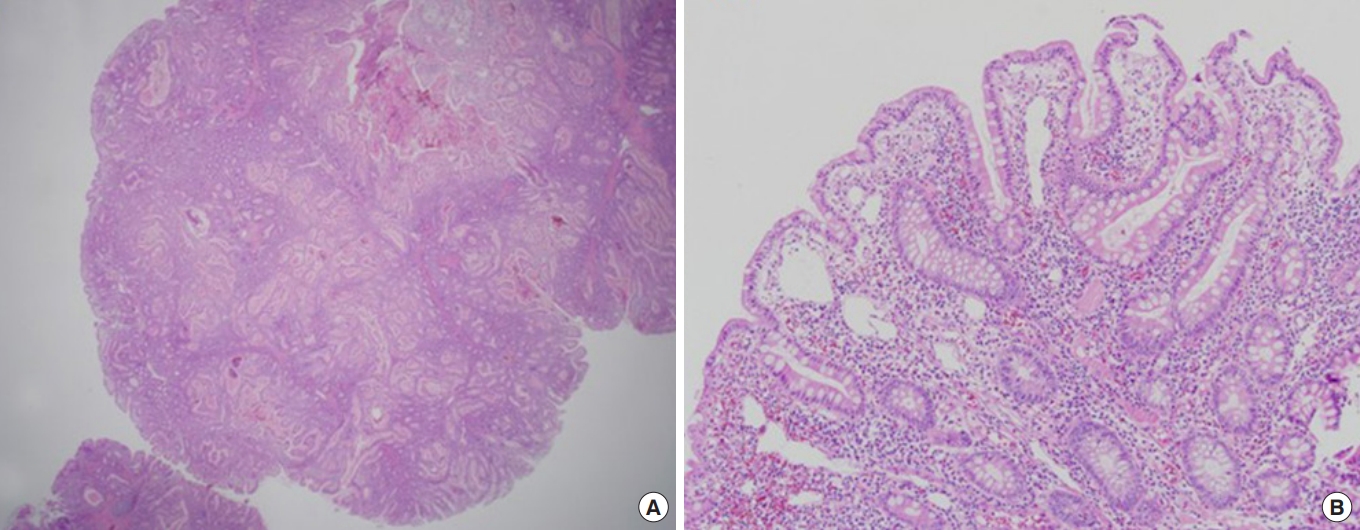
Histopathologic view of the ileal hyperplastic polyp. (A) The proliferation of multiple glands and dilated glands was observed (H&E stain, ×10). (B) Hyperplastic glands without dysplasia, and inflammatory cell infiltration were observed in the stroma (H&E stain, ×100).
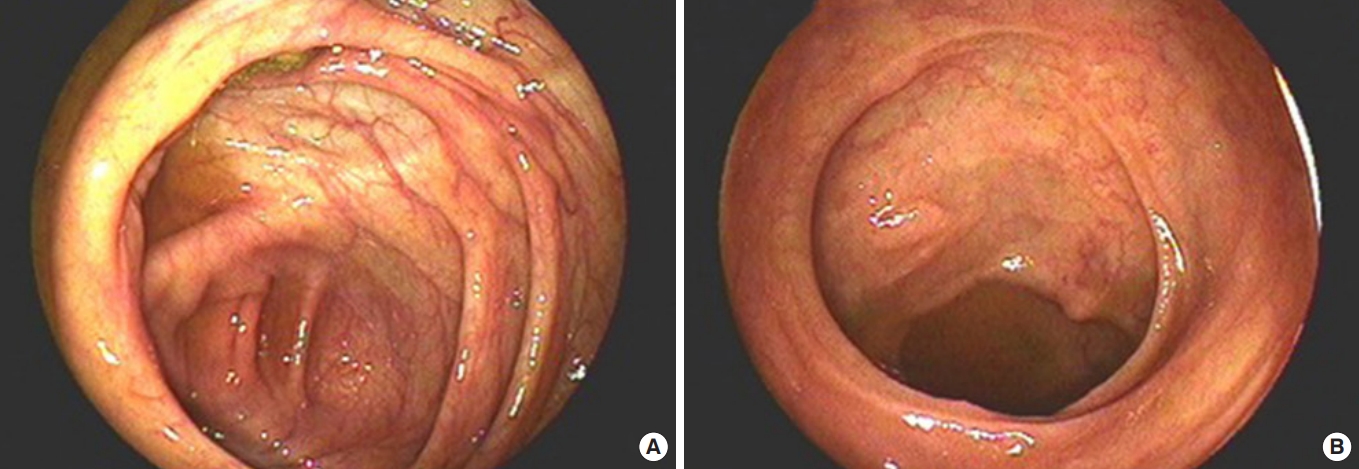
Two years after polypectomy, no recurrence was observed during postpolypectomy surveillance colonoscopy. (A) Cecum, (B) terminal ileum.
DISCUSSION
The small bowel accounts for nearly 75% of the length and 90% of the mucosal surface of the gastrointestinal tract; however, smallbowel tumors are rare, accounting for less than 2% of all malignant gastrointestinal tumors [1, 2]. Recently, the detection of small-bowel tumors has improved because of the introduction of more advanced radiographic and endoscopic approaches to diagnosis. However, small-bowel tumors are difficult to diagnose because of their typically delayed presentation and nonspecific signs and symptoms [3, 4]. Usually, benign small-bowel tumors, including polyps, are asymptomatic and are discovered only at autopsy. However, small-bowel tumors are also commonly found unexpectedly during surgery in patients who present with small-bowel obstruction [1, 4].
The incidence of small-bowel tumors is more common in men than in women with a male preponderance ratio of 3:2, and most patients present with these tumors in their sixth to seventh decade of life [4, 5]. In our case, a polyp of the terminal ileum was found in a 41-year-old male with intermittent right-sided lower-abdominal pain.
Approximately 40 different histologic types of both benign and malignant small-bowel tumors have been identified [1, 2]. Benign small-bowel tumors include leiomyoma, lipoma, adenoma, lymphangioma, fibroma, hamartoma, hemangioma, aberrant pancreas, dermoid cyst, eosinophilic granuloma, angiodysplasia, and hyperplastic polyp [5]. Among them, aberrant pancreas, dermoid cyst, eosinophilic granuloma, angiodysplasia, and hyperplastic polyp are uncommon. In comparison, colorectal hyperplastic polyps are common and well-characterized. However, hyperplastic polyps of the small bowel occur less frequently and have only rarely been studied and described in the literature [6]. Fry et al. [7] subdivided small-bowel polyps into several types, such as hyperplastic polyps, lipomas, sporadic adenoma, familial adenomatous polyposis, familial juvenile polyposis, and polyps associated with Peutz-Jeghers syndrome. In general, small-bowel tumors including only primary tumors are located between the duodenum and the ileocecal valve. That is, the small bowel includes duodenum, jejunum, and ileum. Most of the small-bowel polyps reported so far have been duodenal polyps and diagnosed through esophagogastroduodenoscopy; conversely, our case was detected by colonoscopy [3, 8]. In our experience, polyps of the ileum are rare, with the majority being the inflammatory or lymphoid types. To the best of our knowledge, this report is the first description of a case of hyperplastic polyp of the terminal ileum in Korea.
According to one report, of 23 benign small-bowel tumors, 19 were in the duodenum, 3 were in the ileum, and 1 was in the jejunum; however, only one ileal hyperplastic polyp was observed [3]. Therefore, we believe that ileal hyperplastic polyps are extremely rare. In addition, Irsi and Karacay [9] reported a case of an ileal hyperplastic polyp associated with acute appendicitis found accidentally during exploration to rule out Meckel diverticulitis. We incidentally identified the polyp during colonoscopy in the present case, while these other authors found it in a surgical patient [3, 9].
In our case, although it may be a coincidence, the patient’s intermittent right-sided, lower-abdominal pain improved after polypectomy. Our colonoscopic images show that the polyp could not return to the ileum; therefore, we assumed that it would cause intermittent intestinal obstruction or intussusception, leading to abdominal pain. When the patient visited our clinic, there was no abdominal pain and no abnormal findings were noted during the physical examination of the abdomen at the time. The colonoscopy was performed on the patient’s request. Unfortunately, we did not obtain an abdominal radiograph or a computed tomography scan to confirm this assumption before colonoscopy. In the etiology of intussusception, polyps have an important role, acting as a trigger or leading point [9].
We think that many cases and more research are needed for small-bowel polyps because the 2 terms, small-bowel tumors and small-bowel polyps, have been used interchangeably in various studies, causing confusion.
In general, endoscopic polypectomy for pedunculated tumors and surgical resection for large sessile lesions are appropriate [1]. Endoscopically accessible small-bowel tumors measuring less than 3 cm (in the duodenum, terminal ileum) may be amenable to endoscopic mucosal resection [4]. For small-bowel polypectomy, another report has also recommended the use of a submucosal cushion to prevent perforation whenever possible, especially for all flat lesions, polyps with thick pedicles, and any polyp measuring larger than 10 mm [7]. In our case, the polyp was removed by endoscopic mucosal resection technique without complications. Two years later, there was no recurrence on postpolypectomy surveillance colonoscopy. Currently, many gastroenterologists perform colonoscopy to the terminal ileum, particularly in patients with inflammatory bowel diseases (IBDs) such as Crohn disease and ulcerative colitis; there are, however, endoscopists who do not observe the terminal ileum, especially in patients without IBD. Our patient did not have IBD.
In conclusion, small-bowel polyps, especially ileal hyperplastic polyps, are rare. We report an incidentally detected case of a long, pedunculated, large ileal hyperplastic polyp that was removed by endoscopic mucosal resection using colonoscopy in a 41-year-old male with intermittent right-sided lower-abdominal pain.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.