INTRODUCTION
For the past four decades, the vast improvement in the management of rectal cancer has been achieved based on the development of surgical techniques and the implementation of multimodal therapies. In the early 1980s, the report of ‘Holy plane’ in rectal cancer surgery elaborated a resection technique based on the embryologic development of the hindgut, named total mesorectal excision (TME) [1]. TME resulted in decreased positive circumferential resection margins, which ultimately reduced the local recurrence rate and improved survival outcome dramatically [2, 3]. TME also relegated nonsphincter saving procedure, allowing a majority of patients to save anal sphincter [4].
In a similar timeframe, radiation therapy attracted the attention of many clinicians for treating locally advanced rectal cancer. Several clinical trials were conducted to investigate the effect of radiation therapy in rectal cancer management. The results indicated that the superiority of preoperative radiotherapy for local control with better compliance with treatment and low toxicity [5-8]. Later trials demonstrated the concurrent chemotherapy with fluorouracil and leucovorin given with radiotherapy significantly boosted the local control in locally advanced rectal cancer [9, 10]. These reports also showed an enhanced rate of pathologic complete response and reduced local recurrence rate as low as 5.3%. Therefore, accurately guided by exquisite diagnostic imaging, the multimodal approach using neoadjuvant chemoradiotherapy (nCRT) and subsequent TME is now adopted widely in rectal cancer management.
The current primary approach for managing rectal cancer is a radical resection. It requires high-end surgical training for meticulous TME with nerve-sparing technique. Moreover, radical rectal resection is a major procedure with a substantial risk of perioperative morbidity and mortality, particularly for the elderly [11]. Also, patients who received radical resection cannot avoid ample loss of anorectal, sexual, and urinary function, which eventually leads to poor quality of life [12-14]. As clinical data on patients treated with rectal cancer accumulates, a particular subgroup of patients shows a complete response or non-response to multimodal treatment. This presents a challenge to identify treatment modalities that could maintain or improve the oncological outcome while preserving quality of life.
This article discusses organ preservation strategies after nCRT for managing locally advanced rectal cancer, clinical T3 and above or positive mesorectal lymph node.
NEOADJUVANT CRT AND ADJUVANT CHEMOTHERAPY
It is well known that nCRT can downsize or downstage a tumor, but can also achieve a pathological complete response (pCR) defined as the complete absence of cancer cells in the resected specimen. The rate of pCR is reported up to 10%–32% of patients [15-17]. The prognosis after obtaining pCR is usually excellent, and is often used as a surrogate of oncologic outcome [18]. Two meta-analyses on pCR following preoperative CRT in rectal cancer sought to identify factors that could increase the rate of pCR. These studies revealed that the use of a continuous infusion of 5-fluorouracil, the use of 2 drugs and high radiation doses were associated with higher rates of pCR [16, 17]. Noninferiority, phase 3, randomized trials that compared capecitabine to 5-fluorouracil in CRT showed that capecitabine could be used as an alternative in neoadjuvant or adjuvant CRT regimens [19, 20]. Several other trials also investigated the addition of oxaliplatin to 5-fluorouracil based CRT as a radiosensitizer [20-22]. However, they failed to demonstrate the oxaliplatin as a radiosensitizer but only increased in toxicity; as a consequence, adding oxaliplatin to nCRT was not supported. Finally, although the rate of pCR was higher with increasing doses of radiation, a dose-response effect beyond 45 Gy was not recommended due to the lack of data [16, 17]. In spite of achieving pCR and increasing disease-free survival, nCRT in clinical trials did not reduce the risk of systemic metastasis, and overall survival was not improved [23, 24].
Using the multimodal approach, the rate of local recurrence has been reported atonly 5%–6% in recent years [25], and it seems now less of the concern than developing distant metastasis. Toprevent distant metastases by eliminating circulating tumor cells and micrometastases, adjuvant chemotherapy has been recommended in patients with locally advanced rectal cancer treated with nCRT and TME [26]. This recommendation to patients with stage II or III rectal cancer is based on extrapolation of results from phase 3 trials of adjuvant treatment for colon cancer [27, 28] and data of patients with rectal cancer treated without preoperative radiotherapy or CRT [29]. Based on a systematic review and meta-analysis of adjuvant chemotherapy after preoperative radiotherapy and surgery in patients with rectal cancer, adjuvant chemotherapy for rectal cancer does not improve overall survival, disease-free survival, or distant recurrences in general [30]. In contrast, in patients with upper rectal cancer, adjuvant chemotherapy could be benefitial in terms of disease-free survival and distant recurrence [30]. Therefore, based onthe conflicting data, the benefit of adjuvant chemotherapy remains controversial with regard to clinical application.
In addition, concerns on patient compliance with adjuvant therapy have been raised. Nearly 30% of eligible patients had never initiated adjuvant chemotherapy [31], and less than half of these patients had received the full treatment without interruption or delays [5, 32, 33]. Postoperative complications including leakage, poor general condition, and slow recovery, problems with the temporary stoma, or refusal of treatment were the main reasons for withdrawing from the adjuvant therapy [34]. Evaluation on timing and efficacy of postoperative adjuvant chemotherapy demonstrated that each 4-week delay in treatment correlated with a 14% drop in overall survival [35]. Based on these data, it is clear that poor treatment compliance with adjuvant chemotherapy, regardless of the reasons, impedes patient survival, and other modes of delivering chemotherapy are needed. Therefore, the concept of delivering chemotherapy before surgery has been proposed to treat occult micrometastases earlier and increase treatment compliance, ultimately improving survival outcome [36]. Different methods and schedules for performing systemic chemotherapy before surgery are a current focus in clinical trials in rectal cancer management.
MODE OF DELIVERING SYSTEMIC CHEMOTHERAPY AND pCR
In the effort to improve disease control systemically and locally, induction therapy, dividing adjuvant chemotherapy and delivering a limited number of cycles before nCRT, and then providing the remaining postoperatively has been proposed to increase tumor response in patients with locally advanced rectal cancer [37-41]. Theoretically, upfront chemotherapy allows the chemotherapeutic agents to reach the primary tumor directly when the vasculature is not disrupted either by radiation or surgery, which could optimize the tumor response to the chemotherapeutic agent optimally. The clinical trials of induction chemotherapy demonstrated no adverse effect that delayed treatment, increased pCR rate, and early identification of non-responders along with excellent treatment compliance [16, 18, 36, 42]. The long-term oncologic outcome is not available yet since the therapeutic approach of induction chemotherapy is relatively recent. Based on the short-term outcome of the patients enrolled in clinical trials, the investigators anticipate sufficient survival gains to consider the induction chemotherapy as a viable option for locally advanced rectal cancer [42].
Another way of increasing pCR rate is adding a few cycles of systemic chemotherapy between CRT and surgery, known as consolidation therapy [43]. The results from a nonrandomized, phase II trial showed that consolidation chemotherapy with FOLFOX increased the pCR rate up to 37% while surgical complication was not different from the patients who underwent the standard treatment strategy composed of neoadjuvant chemoradiotherapy, TME, and then adjuvant chemotherapy [43]. Although the overall survival rate was not yet determined from the limited number of patients, the disease-free survival of the patients given to the consolidation chemotherapy during the waiting period for surgery significantly improved [44]. Interestingly, the rate of pCR increased along with the increasing interval between the CRT and surgery while extended cycles of FOLFOX could be given instead of initially intended cycles, as shown in Table 1 [45-47]. As demonstrated by the remarkable compliance of patients along with improved oncologic outcome, the neoadjuvant consolidation chemotherapy after CRT in rectal cancer treatment is another attractive treatment approach for patients with rectal cancer.
The challenges for overcoming the limitations of neoadjuvant CRT in overall survival gain have distinguished a certain patient subgroup with the excellent oncologic outcome. This particular subgroup is presumed to have tumors with distinct characteristics and behaviors that result in a different risk of recurrence and survival probabilities. Diagnostic methods to identify patients that have profiles fortumors with low risk of recurrence and good survival probability are currently under investigation. If applicable, the quality of life in the patient who has rectal cancer may be preserved by skipping a radical rectal resection.
“WATCH AND WAIT” AND “SALVAGE SURGERY”
TME has been the critical element in the multimodal treatment for patients with rectal cancer. However, based on the observation of the clinical and oncologic outcome of patients who obtained pCR after neoadjuvant CRT, some surgeons have contested the multimodal algorithm of neoadjuvant CRT, TME then postoperative chemotherapy. In 2004, the Brazilian group led by Habr-Gama et al. [48] published a retrospective study on the patients managed nonoperatively after achieving significant tumor regression via neoadjuvant CRT, asserting the concept of organ preservation in rectal cancer management. Although the surgical and oncological society predominately reacted with strong objection and skepticism at first, a few years later other groups reported similar findings with a similar therapeutic approach, demonstrating reproducibility [49, 50]. Although these articles exhibited a considerable variation in treatment protocols and nuances of the study population, an organ preservation strategy, particularly for low rectal cancer, has gained the interest of many clinicians and academia, which further supports a focus on avoiding postoperative severe morbidity and poor urinary, sexual, and bowel function after a radical rectal surgery.
In patients with locally advanced rectal cancer, tumor response to nCRT varies widely, and tumor regression grade (TRG) is considered an essential prognostic factor in survival outcome [51]. When a tumor is no longer detectable on various diagnostic modalities including digital rectal exam (DRE), endoscopy, transrectal ultrasonography (TRUS), or magnetic resonance image (MRI), it is referred to as a complete clinical response (cCR), and non-operative management with strict follow-up can be offered [52]. The highest cCR rate after the standard regimen of nCRT, reported by Habr-Gama et al. [53], was 49.2%. Other retrospective studies reported cCR rate from 11% to 16% [54-57]. The discrepancy in the rate of cCR is probably due to different definition and diagnosis of cCR made by investigators as well as the inclusion criteria in each retrospective study. In other prospective studies including T2 and T3 rectal cancers on watch and wait policy, the CR rate, either cCR or pCR, was even much higher, reaching 67.1% to 78.4%, when consolidation chemotherapy or endorectal brachytherapy was given [53, 58].
The incidence of regrowth was reported from 5% to 34%, and most tumor regrowth occurred within the first 2 years [49, 56, 58]. The incidence of systemic recurrence was reported from 5% to 18%, relatively low, accordant with the good prognosis of the patients with pCR [51]. The recently published systemic review and pooled analysis on the oncologic and survival outcome in watch and wait approach demonstrated that the pooled 3-year cumulative rate of local regrowth was estimated to be 21.6%, and the 1- and 2-year cumulative regrowth rates were 11.7% and 18.2% [59]. The pooled 3-year overall survival rate was 93.5%, and the 3-year nonregrowth, the disease-free survival rate was 89.2%. In terms of local recurrence located outside the mesorectal fascia, only 2.7% was reported. The authors suggested that delayed surgery would be feasible in the majority of patients with regrowth. Therefore, the therapeutic option of organ preservation in a particular subgroup of patients with rectal cancer may not be so worrisome.
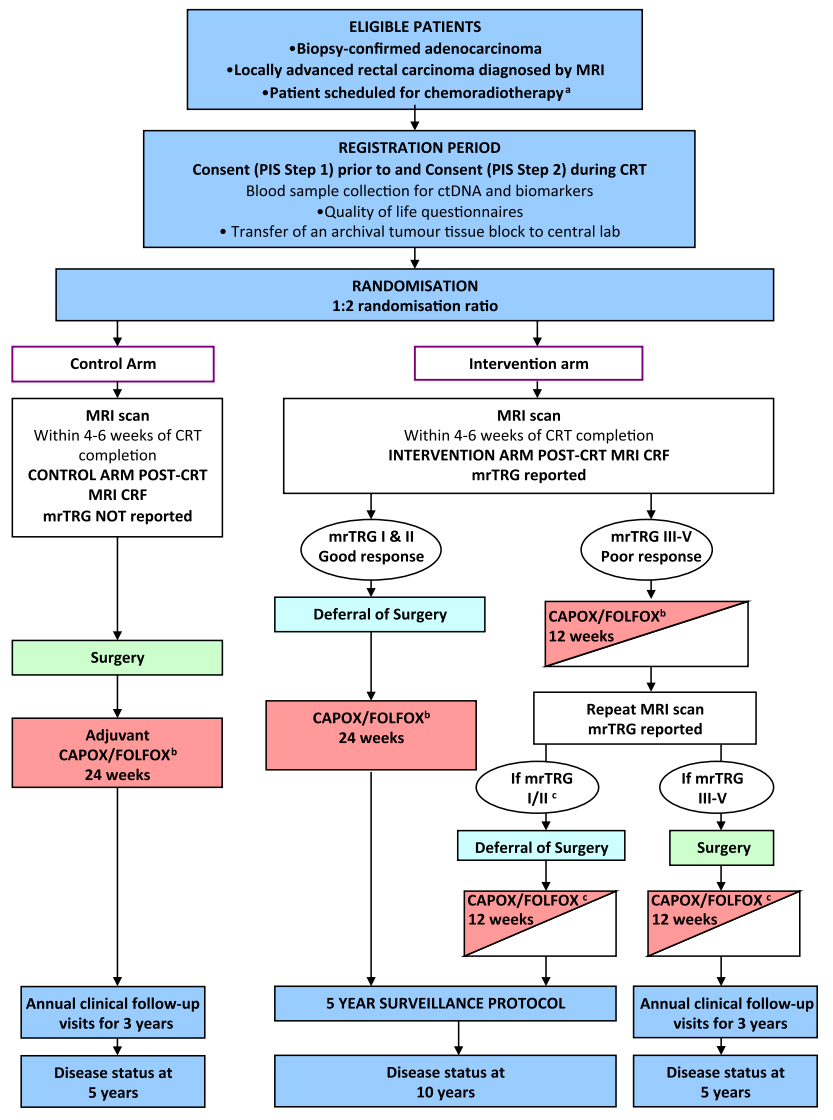
The most critical aspect of the organ preservation approach is the accurate clinical assessment of tumor response and timing of the assessment [52]. The assessment methodology is mostly based on the finding of clinically disappeared tumor mass on DRE and the direct visualization of rectal mucosa left only with scar tissue by endoscopy [48]. Most studies on watch and wait policy reported cCR based on the endoluminal assessment by DRE and endoscopy with or without biopsy [59]. As imaging technology develops, other modalities, including TRUS, abdominopelvic computed tomography, pelvic MRI, 18-fluorodeoxyglucose positron emission tomography (PET-CT), have been used additionally to increase the detection rate of cCR. Development in imaging technique brought out high-resolution MRI which allows for differentiation between fibrosis and residual disease [49, 60-62]. Based on the tumor regression grade measured by MR imaging, the pCR could be identified ten times more, compared with clinical assessment by DRE or endoscopy [63]. However, the value of MRI in restaging after nCRT is still controversial. It is necessary to resolve heterogeneity in the interpretation of various modes of MR imaging technique for restaging rectal cancer after nCRT [64]. The TRIGGER trial, a multicenter, open, interventional, randomized control feasibility study, is ongoing to validate the assessment of tumor response based on MRI-derived tumor regression grading system shortly named magnetic resonance tumor regression grade (mrTRG) [65]. As depicted in the schema of Fig. 1, two prospective subtrials compose the intervention arm based on the mrTRG: the good-response group and the poor response group. The good response group follows the nonoperative approach upfront systemic chemotherapy before surgery. The result of this study will provide a whole lot of vital information regarding the role of MRI in organ preservation strategies for rectal cancer treatment.
Surveillance protocol in watch and wait approach varied greatly in follow-up schedule. Patients were examined in every one to three months by DRE and endoluminal assessment with endoscopy while imaging studies, such as CT scan, MRI or PET-CT scan, were conducted in every 3 to 6 months, shown in Table 2. After the initial assessment post nCRT, patients with cCR were extensively re-assessed in the first two years. The pooled analysis by Dattani et al. [59] demonstrated 61.8% of all local regrowth presented in the first year of surveillance, with diminishing frequency thereafter, such that only 3.8% regrowth were detected beyond 3 years. These data suggest that surveillance protocol for watch and wait approach should include close follow-up during the first 1 to 2 years for observation, and patients should be able to readily adhere to the strict follow-up schedule.
Adding a local excision of the remaining scar can be an option for organ preservation. The advantage would be histological confirmation of a complete response. A multicenterd, nonrandomized trial evaluating the feasibility of transanal endoscopic microsurgery (TEM) in early distal rectal cancer demonstrated TEM could be used for accurate assessment of pathological response in case of a complete clinical response after nCRT [66]. A recent update on the oncological outcome in this CARTS study revealed that the local recurrence in TEM group was not difference from that in TME group, 9% vs. 7.7%; the 5-year disease-free survival for TEM group was 81.6% [67]. Also, a randomized controlled trial comparing the oncological outcome of TEM to laparoscopic TME for the treatment of patients with clinical stage T2 N0 M0 after nCRT suggested TEM had similar local recurrence rate, systemic metastasis, and disease-free survival [68]. However, a systematic review and meta-analysis on local excision after nCRT in early rectal cancer demonstrated local recurrence exceeded 20% in local excision group, and the authors implied probably reduction in long-term survival for the patients who did not achieve pCR [69]. In this review, the pooled local recurrence for ypT0 was 4%, but rising to 12.1% for ypT1 and 23.6% for ypT2 tumors. Therefore, the authors insisted that for oncological safety, local excision alone should only be considered a potential curative treatment if a pCR has been obtained.
Besides the oncological safety, other issues regarding local excision after nCRT include toxicity from chemoradiation therapy and postoperative complication arising from the unhealing rectal wound after nCRT. In current standard of care, early rectal cancer does not require nCRT before surgery. However, previous studies had reported mortality after nCRT, owing to toxicity from nCRT [66, 70]. Also, patients reported grade 3 to 4 toxicity during nCRT [66]. Thus, giving nCRT to patients with early rectal cancer should carefully be reviewed about possible chemotoxicity and necessity of radical surgery in case of poorly responsive tumor.
The incidence of postoperative complication and morbidity was 23.2% in the overall pooled data [69]. The most frequent complications were suture line dehiscence and rectal pain with the rate of 10%. Among them 13.7% required operative re-intervention including diverting loop stoma, transanal re-suturing, anal stenosis, transsacral wound debridement, and abdominoperineal resection [69]. A prospective study on the postoperative outcome after TEM following nCRT in cT2 and T3 rectal cancer reported 44% immediate complication of Clavien-Dindo classification grades II and III including rectal pain, bleeding, fistula, and peritonitis, and the hospital readmission rate was 30% [71]. In this report, the wound dehiscence was observed in 47%. Late complication arising after postoperative 30 days was also reported, which included stenosis requiring general anesthesia for rectal dilatation and seminalvesicle fistula treated with oral antibiotics. The authors warned of that the use of TEM after nCRT would result in a significant morbidity, sometimes requiring invasive procedures. Altogether, local excision after neoadjuvant CRT as an organ-preserving strategy in rectal cancer treatment may play a role in highly selected patients. However, considerable morbidity from local excision and possible mortality from chemoradiation should be accounted before offering.
As previously discussed, the risk of regrowth is high in the first two years. If regrowth is detected, the standard treatment is TME [72]. The investigators studying organ preservation strategy insist that local regrowth detected early with sufficient follow-up can be treated adequately by salvage surgery [72]. A recently published systematic review on the outcome and salvage surgery following organ-preservation strategy shows that 69.2% of “watch and wait” group exhibited persistent cCR, and salvage surgery was possible in 83.8% in patients who developed tumor regrowth [73]. Although the overall survival and disease-free survival between patients who received immediate surgery and the “watch and wait” group was not different, the authors concluded that the evidence is insufficient to draw a firm conclusion on the oncological safety of the current organ preservation strategy. Other experts express a similar opinion on the previous studies on organ preservation approach, criticizing the significant heterogeneity of data and methods of research [74].
Furthermore, delaying surgery may impose detrimental effect in the patients who require surgical treatment after neoadjuvant CRT. A multicentered, randomized trial, GRECCAR-6 trial, investigated the effect of increasing the delay period between nCRT and surgery [75]. The investigators found that increased morbidity and a poor quality of TME was seen in the patients in longer waiting period of 11 weeks compared to the patients in standard waiting period of 7 weeks. They concluded that a longer waiting period may be associated with higher morbidity and more difficult surgical resection. The optimal interval for waiting period and timing for re-assessment is unanswered. Further research is needed to determine the risk and benefit of prolonged interval between nCRT and surgery.
Salvage TME for the regrowth after full-thickness local excision seems to impose a significant threat, jeopardizing the oncologic principle. A retrospective study on patients who underwent salvage TME after nCRT and subsequent local excision demonstrates that salvage TME was associated with 87.5% of circumferential resection margin positivity and 40% of the local re-recurrence rate at two years [76]. Fibrosis and scar tissue may disrupt the surgical plane, extending into or beyond the mesorectal fascia; thus, the optimal TME cannot be achieved when it’s needed [72]. Whether or not the salvage TME is sufficient for surgical and oncological outcome remains to be clarified.
TOTAL NEOADJUVANT THERAPY AND ORGAN PRESERVATION
The National Comprehensive Cancer Network (NCCN) guidelines for locally advanced rectal cancer have recommended a multidisciplinary approach with neoadjuvant CRT followed by a radical surgery, with TME principle approach, then adjuvant chemotherapy [26]. However, as mentioned before, due to low compliance and uncertain survival benefits of adjuvant chemotherapy, many clinicians and researchers have planned trials to test the “total neoadjuvant therapy” approach, in which all planned radiation therapy or chemotherapy is delivered preoperatively [77]. Combining induction and consolidation chemotherapy with oxaliplatin-based regimen along with oral or intravenous 5-FU seems to improve the pCR rate and compliance without a significant increase in the toxicity [41, 42, 44, 77-80]. Other randomized controlled trials, such as the TRIGGER trial [65], the RAPIDO trial [81], a phase II trial by MSKCC [82], the KONCLUDE trial [83], and others [84-86], are ongoing to find a feasible and effective regimen that achieves good oncologic outcome and high organ preservation rate, as shown in Table 3. These trials are anticipated to provide better understanding of tumor characteristics and behavior, which will lead to the development of selection criteria for patients that are the optimal candidate for organ preservation. One caution of delivering total neoadjuvant therapy is that the potential to increase toxicity should be carefully addressed.
CONCLUSION
The idea of organ preservation in rectal cancer management is a radical concept which alters the fundamental belief of anatomical eradication in cancer treatment. Tremendous interest and desire for organ preservation in rectal cancer are partly driven by the yearning of patients who want to preserve a decent quality of life in the modern era. A large volume of concurrent evidence that organ-preservation strategy is as safe as stand TME is currently lacking. Clinicians and surgeons should carefully follow the evidence to advisee individual patient, offering the most reliable treatment option that satisfies the need of patients. Upcoming results from multiple ongoing and future trials are anticipated to provide insight for clinical decisions about the optimal oncologic outcome as well as improved quality of life.