INTRODUCTION
The subdivisions of colorectal cancer and the T staging system have been extensively investigated due to the premise that poorer prognoses are correlated with the depth of tumor invasion [1]. This issue was first raised by the International Documentation System and the International Comprehensive Anatomical Terminology in 1991 [2]. About a decade later in 2003, a T3 optional subdivision was proposed by the Union Internationale Contre le Cancer [3-6].
In 2001, a proposal regarding the division of T3 cancers into two subgroups based on a standard 5-mm depth of invasion into the muscularis propria was made [7]. This proposal was practiced in selected groups to predict both prognosis and local recurrence [4, 6]. In spite of these trials, the subdivision of T3 was not adopted by the American Joint Committee on Cancer (AJCC) in 2002 [8] and in 2010 [9], and it still has not been applied as the standard in the United States [9, 10]. Meanwhile, the subdivisions of T4a and T4b, presented by the AJCC in 2010, were based on accumulated data [9]. To clarify the ambiguity of T3 colon cancer prognoses, supplementing the existing tumor-node-metastasis (TNM) system to improve the success rate of medical treatments for these tumors is important [4, 5, 7]. The aim of this study is to assess whether the T3 subdivision correlates with node (N) or metastasis (M) staging and other stage-independent factors.
METHODS
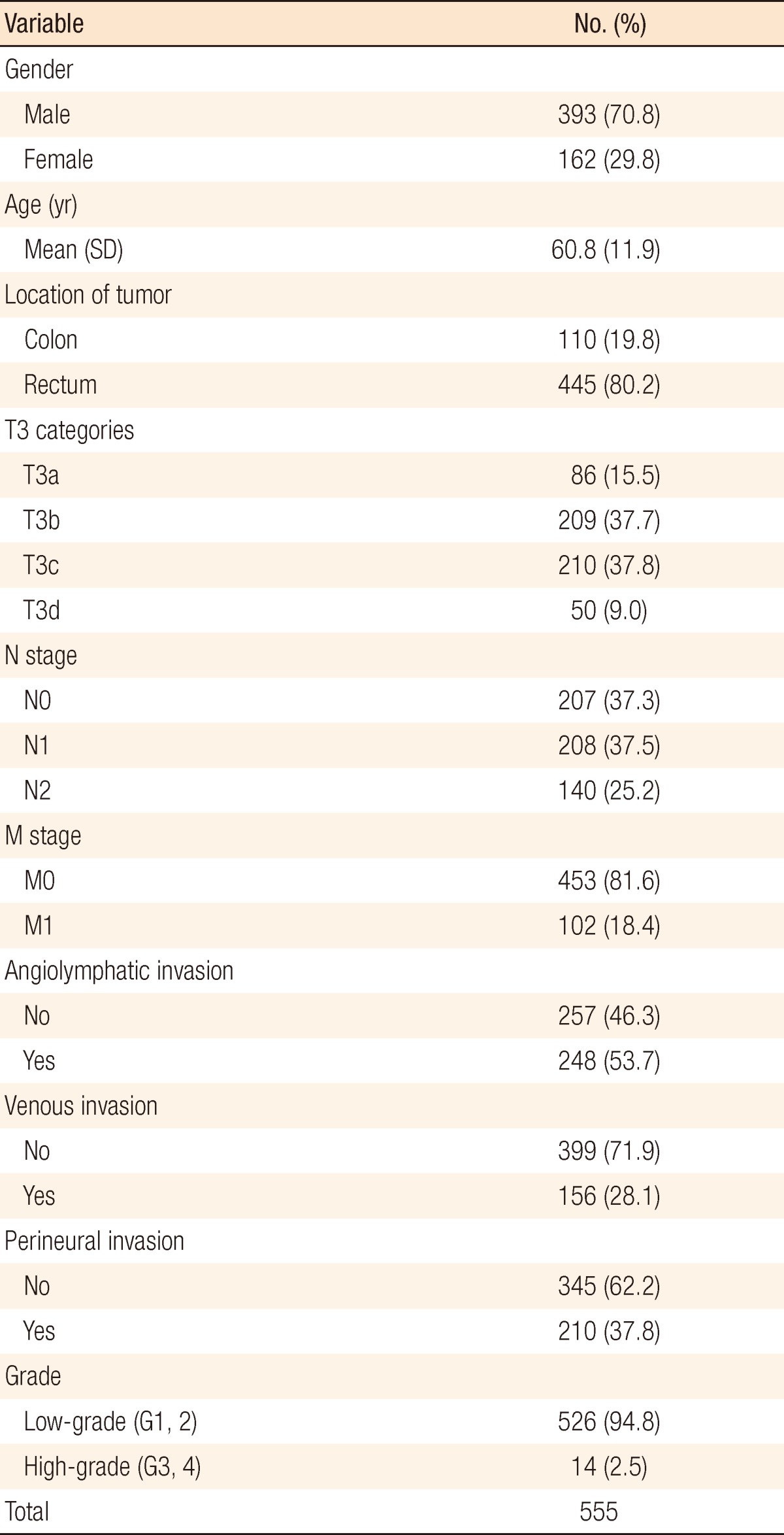
We retrospectively reviewed clinicopathologic records of 592 patients who had undergone surgery for a pathologically proven T3 primary colorectal adenocarcinoma with valid information on the T3 subclassification at the Department of Surgery, Seoul National University Hospital, between January 2003 and December 2009. Among them, we excluded patients with hereditary nonpolyposis colorectal cancer (n = 4), familial adenomatous polyposis (n = 7), and synchronous or metachronous malignancies other than colorectal cancer (n = 26). Finally, 555 patients (393 men and 162 women; mean age, 60.8 ┬▒ 11.9 years; range, 23 to 91 years) were included for analysis.
The category of pT3 was subdivided according to the histological measurement of the maximal tumor invasion beyond the outer border of the muscularis propria (T3a, <1 mm; T3b, 1 to 5 mm; T3c, >5 to 15 mm; T3d, >15 mm). The specimen slide was observed at a magnification of 40 times. An imaginary line was drawn horizontally extending from the normal muscularis propria next to the lesion. The depth of the lesion infiltrating under that line was measured. Fig. 1 shows the pathologic specimens of T3a, T3b, T3c and T3d tumors. Clinico-demographic and the histopathologic parameters, including the location of the tumor, histologic type and grade, angiolymphatic invasion (ALI), venous invasion (VI), perineural invasion (PNI) and tumor stage, were retrospectively reviewed. Tumor stage was determined using the 6th AJCC TNM system [8]. Tumor grade was categorized as low-grade (well or moderately differentiated) and high-grade (poorly differentiated, anaplastic, or undifferentiated). The stage-independent factors were classified using two categories: no invasion and invasion [11].
Correlations among the aforementioned factors were based on Spearman correlation analyses (Spearman correlation coefficient). A perfect Spearman correlation of +1 or -1 occurs when each variable is a perfect monotone function of the other. P-values less than 0.05 were regarded as statistically significant. All of the statistics were performed using IBM SPSS ver. 19 (IBM Co., Armonk, NY, USA).
RESULTS
Patients and tumor characteristics
For the 555 patients, tumors were subclassified as T3a in 86 (15.5%), T3b in 209 (37.7%), T3c in 210 (37.8%) and T3d in 53 (9.0%) patients. Clinicopathologic characteristics of the patients are listed in Table 1. Lymph node metastasis was found in 62.7% of the patients and distant metastasis in 18.4% of the patients. The mean number of harvested lymph nodes was 16.8 ┬▒ 9.9. Curative surgery was performed in 87.6% of the patients. Overall stagings of the patients were IIA in 197 (35.5%), IIIB in 178 (32.1%), IIIC in 102 (18.4%), and IV in 78 (14.1%) patients.
Correlation between T3 subdivision and N and M stages
The rate of lymph node metastases increased in the advanced T3 subdivision (Table 2). The nodal stage correlated well with T3 subdivision (Spearman's rho = 0.288, P < 0.001). The distant metastasis rates were 7.0% for T3a, 9.1% for T3b, 27.1% for T3c, and 40.0% for T3d lesions. M stage also correlated well with the T3 subdivision (Spearman's rho = 0.276, P < 0.001).
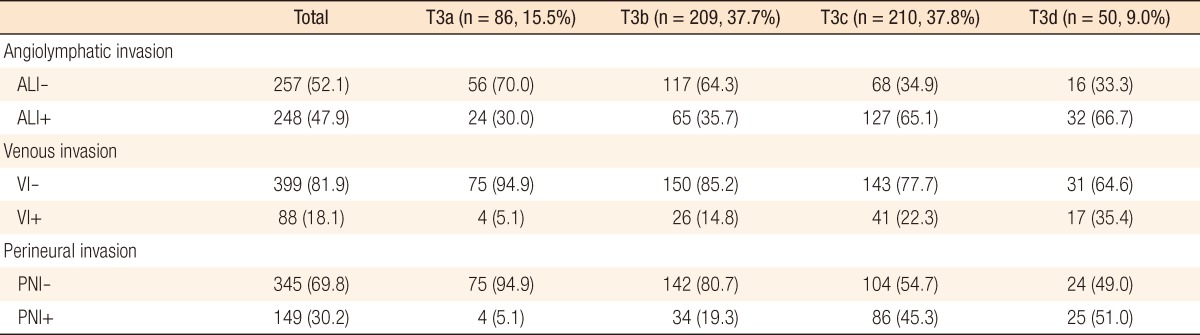
Correlation between T3 subdivision and stage-independent factors
The correlation coefficients (Spearman's rho) between the T3 subdivision and stage-independent factors were 0.250, P < 0.001 for ALI; 0.146, P < 0.001 for VI; 0.271, P < 0.001 for PNI. T3 subdivision also demonstrated a tendency to have a positive linear correlation with stage-independent factors. As the stage advanced, the percentage of ALI, VI and PNI increased (Table 3).
DISCUSSION
The recent boom of personal health check-ups and the popularization of colonoscopy have facilitated detection of early-stage colorectal cancer, but still the majority of patients encountered in clinics have advanced tumors. From 2003 to 2009, 3,913 patients underwent surgery for colorectal cancer at the Department of Surgery, Seoul National University Hospital. Among them, the majority of patients (68.2%) had tumors that had invaded beyond the muscle layers (T3, 2,309 patients [59.0%]; T4, 360 patients [9.2%]). Although T3 tumors occupy more than half of all cancers, they are classified as only one stage whereas T4 tumors are divided into two groups, T4a and T4b.
Several reports have demonstrated a prognostic heterogeneity among T3 colorectal cancers. Some authors indicated the depth of extramural fat invasion as a significant prognostic factor [3, 5, 12-17]. In 2001, the Erlangen Registry of Colorectal Carcinoma (ERCRC) and Study Group for Colorectal Carcinoma (SGCRC) Studies proposed that the perimuscular invasion should be subdivided into Ōēż5 mm, 5 mm to 15 mm, and Ōēź15 mm according to the histological measurements. T3 tumors were subdivided into T3a and T3b by using a 5-mm cutoff point for invasion depth of T3 tumors in stage II colon cancer. The local recurrence rate was shown to be significantly higher for T3b tumors than for T3a tumors in the ERCRC data, but a similar result was not demonstrated in the SGCRC data [7, 12]. Willet et al. [5] subdivided T3 lesions into 3 groups by using the depth of invasion: <2 mm, 2 to 8 mm, and Ōēź8 mm, and they demonstrated a significant difference in the recurrence-free survival (87% vs. 57% vs. 36%, respectively).
In addition, various prognostic cutoff points such as 3 mm, 4 mm, and 6 mm have been proposed for the subdivision of T3 colorectal cancer [3, 13, 14]. Furthermore, by using a univariate analysis, Burdy et al. [18] showed that mesocolic invasion of more than 1 cm was significantly associated with a higher risk of tumor recurrence in T3-4 node-negative colon cancer. Although multivariate analysis showed that other factors were also independently associated with tumor recurrence, that the depth of mesocolic invasion has been considered as a significant predictive factor for tumor recurrence is meaningful.
The depth of local tumor invasion remains as an independent and significant prognostic factor even in the presence of lymph node metastasis. Lymph node metastasis has been recognized as the main clinical indicator for predicting survival in curatively-resected colorectal cancer [19]. Several reports demonstrated that the extent of the primary tumor was related with nodal metastasis, distant metastasis, or stage-independent prognostic factors. Wong et al. [20] explored whether depth of invasion held important prognostic importance both in the presence and the absence of nodal or distant metastases in colon cancer. They demonstrated that the depth of local tumor invasion correlated strongly with nodal involvement, rates of extramural VI, poor differentiation, and distant metastasis. In patients with lymph node or distant metastasis (43%), the depth of tumor invasion had a significant impact on overall survival [20]. In this study, all T-staged colorectal cancers were included and were divided according to the conventional TNM system.
In the present study, we demonstrated that the T3 subdivision had a statistically significant correlation with other factors, including N and M staging, but that the correlation coefficients were not so high. This implies that several other factors that influence the tumor biology and the oncologic outcomes may exist. To date, many studies have focused on finding surrogate markers for the prognosis of colorectal cancer, and many of them included molecular markers. Mutch [21] advocated that tumor staging and molecular markers, including gene expression profiling, have significant correlations and that these molecular markers should be incorporated in a future staging system. However, due to the cost and the technical complexity in evaluating these markers, not every clinic has the capability of testing for the "new" markers.
The stage groups within the TNM classification are divided according to the overall survival rates, and nodal and distant metastasis differentiates stage III from IV. The TNM classification stratifies patients according to the risk of recurrence or metastasis and identifies patients who will benefit from more aggressive adjuvant therapy. Therefore, elucidating clinicopathologic factors that have correlations with lymph node or distant metastasis is important. Especially, factors that can be easily evaluated, such as tumor invasion depth in the present study, have greater usefulness.
In conclusion, we demonstrated that subdivision of T3 colorectal cancer correlates well with nodal and metastasis staging. It also correlates well with other already known prognostic factors for colorectal cancer. We can postulate that invasion depth may influence the prognosis for patients even when they have the same T3-staged tumors, but this should be further verified with a future study on patient survival and recurrence.