INTRODUCTION
Preoperative chemoradiation therapy (preop-CRT) followed by total mesorectal excision (TME) has gained popularity in the treatment of locally advanced rectal cancer. Tumor response after preop-CRT for rectal cancer varies considerably, with some entities showing a complete absence of viable tumor cells and other entities exhibiting a mass of tumor cells with little or no regressive change. Recent studies have demonstrated that good response to preop-CRT in itself is a favorable prognostic factor [1-4]. Therefore, an accurate evaluation of tumor response to preop-CRT is considered essential for predicting oncologic outcomes and planning further treatment.
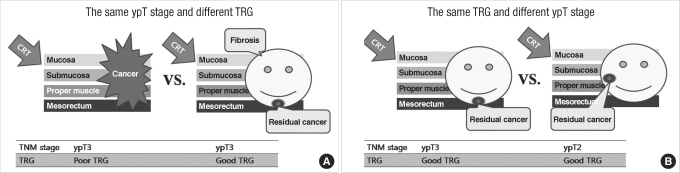
The assessment of histopathologic T and N (ypT and ypN) stages remains as the gold standard for evaluating response to preop-CRT and predicting prognosis. Histopathologic T and N downstaging effects have been recognized as important factors for determining long-term prognosis. Histopathologic downstaging of rectal cancer after chemoradiation is associated with an increased resectability and more chance of anal sphincter preservation. It is also associated with improved local control and long-term survival [2]. Especially patients who show pathological complete response (pCR; complete absence of tumor cells) after the therapy are found to have excellent oncologic outcomes [5-7]. Kim et al. [8] also analyzed the oncologic results of 114 patients who received preop-CRT for locally advanced rectal cancer. They also observed that pCR was related to excellent oncologic outcome and that histopathologic N downstaging was the most important prognostic factor. However, ypT and ypN stages do not provide any information about postirradiation changes in tumors, such as the remaining portion of viable cancer cells. For example, patients with small islets of viable cancer cells scattered in the subserosa layer showing predominant fibrosis are still documented as having a ypT3 tumor, but their prognosis might be different from the prognosis given to patients with a poorly responding pT3 tumor in which most of cancer cells remain viable (Fig. 1A).
The tumor regression grade (TRG) originally proposed by Mandard et al. [9] is assessed by examining the residual neoplastic cells and scoring the degree of both cytological and stromal changes, including necrosis, eosinophilia and fibrosis in esophageal cancer, following preoperative chemoradiation therapy. They showed through a multivariate analysis that TRG was a significant prognostic factor for 3-year disease-free survival. Ruo et al. [10] reported the oncologic outcomes of 69 patients who had been initially diagnosed as having cT3-4/N1 rectal cancers and who had undergone preop-CRT. They observed that patients showing high degrees of tumor regression tended toward good long-term outcomes. Although the TRG designates the histopathologic regression of tumors in response to radiation, it does not provide any information about nodal metastasis or the depth of tumor invasion (Fig. 1B). Thus, despite abundant previous research, whether or not the extent of primary tumor regression has as significant impact as histopathologic downstaging remains inconclusive.
The aim of this study was to investigate the prognostic significance of a semi-quantitative grading system for tumor regression after preop-CRT. We first performed analyses for all patients and then for the subgroup of the patients who had no lymph node metastasis (ypN0). We also investigated whether TRG had any correlation to the presence of metastatic lymph node or to histopathologic T- and N- downstagings, all of which are known to be the most powerful prognostic factors. Finally, we investigated whether different prognoses were observed among the ypN0 patients with different TRGs given a specific ypTN stage or vice versa.
METHODS
Eligibility
Between January 1994 and December 2003, 206 consecutive patients underwent preop-CRT, followed by surgical resection, for the treatment of a carcinoma of the rectum at Severance Hospital, Yonsei University Health System. Those patients were confirmed as having an adenocarcinoma of the rectum by using a rigid sigmoidoscopic biopsy and as having a stage T3 or T4 tumor as defined on transrectal ultrasonography (TRUS) and pelvic magnetic resonance imaging (MRI), regardless of lymph node metastasis. The cN stages were decided on the basis of TRUS, computed tomograph (CT), and MRI findings. cN (+) was defined as enlarged (Ōēź 10 mm) or spiculate lymph nodes being seen on any preoperative imaging examinations. Digital rectal examination showed fixed mass lesions, and initial radiologic evaluation by pelvic MRI revealed bulky tumors, highly suspicious of an invasion of the mesorectal fascia or adjacent organs. Distant metastasis was excluded in all cases by chest X-radiography and abdominopelvic CT. Excluded from the study were 28 patients who had undergone a palliative resection (R2) due to incidentally found distant metastases or to unresectable primary tumors determined at the time of operation. A total of 178 consecutive patients who underwent a curative resection for locally advanced rectal cancer after preop-CRT were prospectively observed, and their clinical and histopathologic data were collected and analyzed.
Preoperative chemoradiation
All enrolled patients received preop-CRT. Preoperative radiation therapy of 45 Gy/25 fractions was delivered to the pelvis, followed by a 5.4 Gy boost to the primary tumor over a period of five weeks (1.8 Gy for five days) by using linear accelerators with an energy of 10 MV. Chemotherapy was administered concurrently with radiotherapy and consisted of intravenous bolus injection of two cycles of 5-fluorouracil (425 mg/m2/day) and leucovorin (20 mg/m2/day) for five days at both the first and the fifth weeks of radiation therapy. The radiation field was as follows: the upper margin was 1.5 cm above the sacral promontory (L5 level), and the lateral margin was 1.5 cm lateral from the bony pelvis in order to include the pelvic lymph nodes. Postoperative adjuvant systemic chemotherapy, consisting of 400-425 mg/m2 of 5-fluorouracil plus 20 mg/m2 leucovorin for 5 days, was administered every 28 days for four cycles in all enrolled patients.
Surgical resection
Surgery was performed 4 to 6 weeks after the completion of chemoradiation. The method of operation was a tumor-specific mesorectal excision with pelvic autonomic nerve preservation. A tumor-specific mesorectal excision is defined as a surgical method in which the rectum is transected with the surrounding mesorectum enclosed by the rectal proper fascia at 4 cm distal from the lower edge of the rectum. Thus, all surgeries were performed using a sharp pelvic dissection under direct vision along the plane of the rectal proper fascia. A tumor-specific mesorectal excision was performed according to each patient's tumor level. In upper rectal cancers, the mesorectum was excised 4 cm distal from the lower edge of the tumor. A total mesorectal excision was performed in middle and distal rectal cancers.
Histopathologic evaluation
Following surgery, pathologic analyses of the tumor specimens were performed. ypT and ypN stages and TRG of all enrolled patients were documented by two pathologists (JYP and HK) who had not been informed of the patients' clinical information. Irradiated cancer and harvested mesorectal lymph nodes were submitted for microscopic analysis. Hematoxylin-eosin-stained sections were reviewed, and proximal, distal, and circumferential resection margins were evaluated. A careful search of the mesorectum was performed to identify as many lymph nodes as possible. In cases where only acellular pools of residual mucin were noted, the response was considered to be complete. The resected specimens were staged according to the 6th American Joint Committee on Cancer (AJCC) TNM staging system [11].
The resected specimens were fixed in 4% formaldehyde overnight. After a specimen had been opened, the tumourous or fibrotic area was identified and described macroscopically. For an obvious residual primary tumor, a minimum of four paraffin blocks were processed. If no tumor was visible, the whole area suggestive of disease was sliced and embedded. The TRG was semiquantitatively determined by two pathologists uninformed of the clinical or radiologic findings. If there were discrepancies between the pathologists, the worse results were selected. Regressive changes of the primary tumors in response to preop-CRT were documented as described by Mandard et al. [9] Regressive changes included both cytological changes, such as cytoplasmic vacuolization and/or eosinophilia, nuclear pyknosis, and necrosis, and stromal changes, such as fibrosis, with or without inflammatory infiltrate. On the basis of these changes, primary tumor regression was grouped into three categories as suggested by Rodel et al. [6]: Grade 1 (complete regression) showed an absence of histologically identifiable residual cancer, with predominant fibrosis extending through the different layers of the rectal wall. Grade 2 (intermediate regression) was characterized by an increase in the number of residual cancer cells, which was still outgrown by fibrosis. Grade 3 (poor regression) showed residual cancer outgrowing fibrosis characterized by a scant presence or the complete absence of regressive changes and by residual cancer cells.
Tumor downstaging was assessed by comparing the pre-CRT clinical stage (cT and cN stage) with the postoperative histopathologic stage (ypT and ypN stage). T-downstaging was defined as the ypT being lower than cT, and N-downstaging was defined as cN (+) converting to ypN0. We simplified the cN stages into cN (-) and cN (+) because detailed categorization of cN stages has been reported to be related with lower accuracy [12] and may cause further bias in determining N-downstaging.
Postoperative follow-up
All patients were closely followed by the surgeons, medical oncologists, and radiation oncologists in the Colorectal Cancer Clinic at our institution. Postoperative follow-ups on all patients were conducted every three months for three years. Clinical examination, measurement of serum carcinoembryonic antigen (CEA) levels, and chest X-rays were performed during each follow-up. After three years, patients underwent follow-up examinations every six months. Abdominopelvic CT and whole body bone scans were taken at the postoperative sixth month for the first time and then every year. An additional pelvic MRI was taken when a routine CT scan failed to discriminate suspicious lesions in the pelvic cavity. The mean and the median follow-up periods were 42.9 ┬▒ 28.3 months and 39 months, respectively.
Statistical analysis
We performed analyses on the association of TRG with histopathologic stages, including T- and N- downstagings, and analyzed the prognostic factors for survival and recurrence by using univariate and multivariate methods. Subgroups classified according to ypT and ypN stages and TRG were analyzed to determine the prognostic impact of TRG for each subgroup.
One-way analysis of variance testing was used to compare continuous variables. When comparing ordinal categorical variables with nominal ones, the Žć2 test for trend was used, and for the comparison of nominal categories, the ordinary Žć2 test was used. The distribution of ordered categories was analyzed by using the Spearman correlation coefficient test. Cancer-specific survival, time to local recurrence and time to systemic recurrence were measured from the time of operation. Data from the patients who were alive regardless of recurrence or who had died without recurrence were not considered in the analysis of CSS. The Kaplan-Meier method was used for the univariate analyses of survival, and the log-rank test was used for the evaluation of differences. The multivariate analyses were carried out by using the Cox-proportional hazards model. A two-sided P value of less than 0.05 was considered significant. An adjustment for multiple testing was performed with the Bonferroni method. All statistical tests were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics and the correlation of TRG with clinical parameters
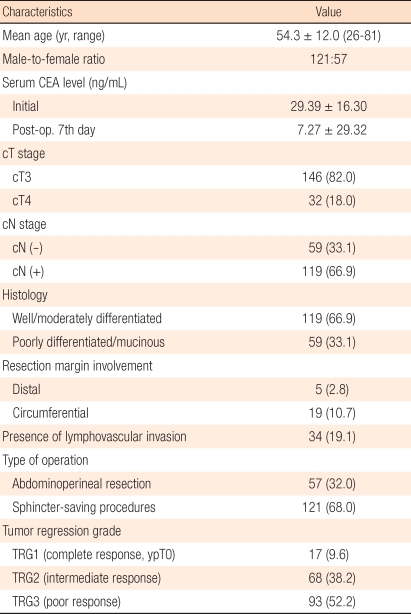
Patient characteristics are summarized in Table 1. Patients with complete regression of their primary tumors (TRG1) had a significantly younger mean age than the other TRG groups (P = 0.006). The initially small tumors showed a significant tendency to show better response to preop-CRT (P = 0.001). Other clinical parameters, such as gender, histology, resection margin involvement, lymphovascular invasion, serum CEA levels, initial (before preop-CRT) clinical T and N stages, tumor location, and sphincter preservation, were not related to TRG.
Correlation of TRG with histopathologic stages
Given the facts that TRG1 was ypT0 and that ypT0 means T-downstaging (+) by definition, the assessment of the relationship of TRG with ypT stage and T-downstaging was performed excluding the TRG1 group. Although advanced ypT stages were noted frequently in the group of patients with TRG3 compared to the groups of patients with TRG2 (r = 0.384; P < 0.001), T-downstaging was found not to be related to TRG (P = 0.326) (Table 2). TRG was found to have significant correlations with both the ypN stage (P = 0.011) and histopathologic N-downstaging (P = 0.007). Two out of 17 patients (11.7%) with TRG1 showed lymph node metastasis.
Prognostic significance of TRG for the whole and the subgroup of ypN0 patients
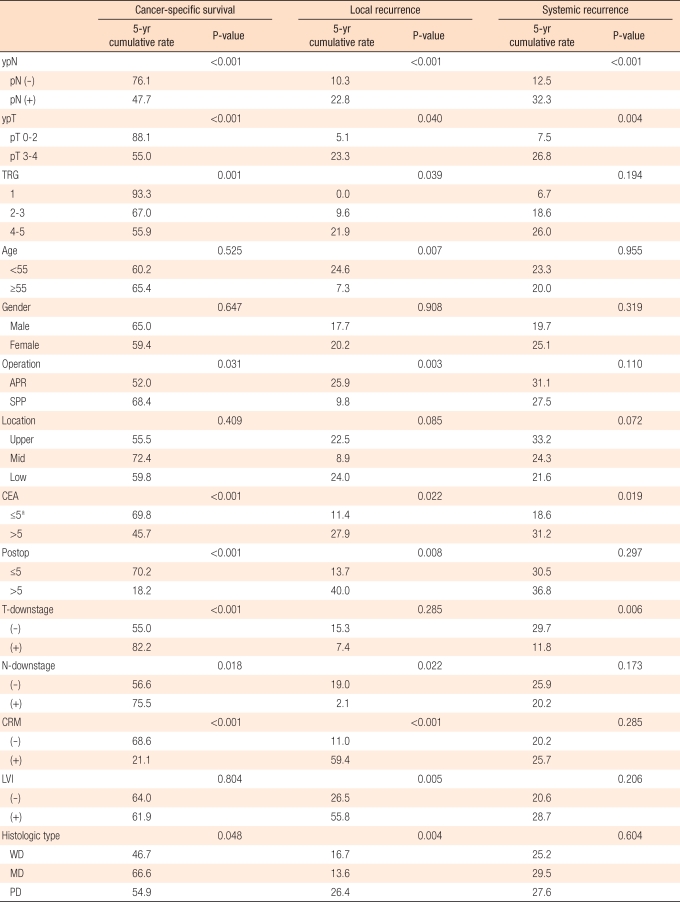
The 5-year cumulative rates of CSS, local recurrences (LR), and systemic recurrences (SR) according to histopathologic stages and TRG are summarized in Table 3. During the follow-up period, local recurrence was observed in 26 patients (14.6%), systemic recurrence in 30 patients (16.9%) and simultaneous local and systemic recurrence in five patients (2.8%).
At first, univariate and multivariate analyses of prognostic factors were performed for all patients. The univariate analysis revealed that TRG was significantly correlated with CSS (P = 0.001) and LR (P = 0.039). TRG was found not to be associated with SR. The ypT and the ypN stages were significantly associated with CSS (P < 0.001, P < 0.001), LR (P = 0.040, P < 0.001), and SR (P < 0.001, P = 0.004). Histopathologic T-downstaging was found to be associated with CSS (P < 0.001) and SR (P = 0.006), and N-downstaging was significantly associated with CSS (P = 0.018) and LR (P = 0.022) (Table 4). Of those histopathologic variables and TRG, the ypN stage was found by multivariate analysis to be the strongest independent prognostic factor for all three endpoints (for CSS: P = 0.007, HR = 2.867, 95% CI, 1.325 to 6.202; for LR: P = 0.002, HR = 11.111, 95% CI, 2.433 to 50.613; for SR: P = 0.003, HR = 3.131, 95% CI, 1.474 to 6.651) (Table 5).
We performed univariate and multivariate analyses for the subgroup of the patients without lymph node metastasis (ypN0). Although univariate analyses showed that ypT stage (P = 0.002) and TRG (P < 0.001) were both significantly associated with CSS (Table 6), on the multivariate analysis, only TRG was found to be an independent prognostic factor for CSS of the patients with ypN0 rectal cancer (P = 0.031) (Table 7).
Survival analyses given a specific TRG and histopathologic stage
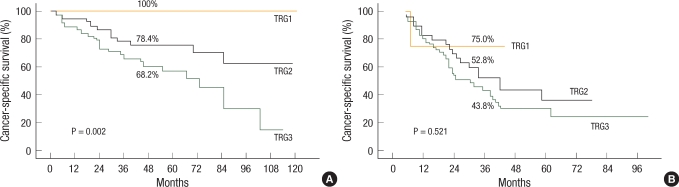
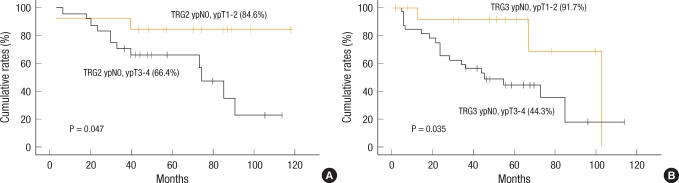
When the patients were split into ypN0 and ypN1-2 groups, TRG classification correlated significantly only with the CSS of patients with ypN0 tumors (P = 0.002) (Fig. 2). Thus, further analysis was focused on the CSS of patients with ypN0 tumors. When given a specific ypT stage (i.e., ypT2 or ypT3), the CSS of the patients was found to be significantly different according to TRG (P = 0.041 for ypT2 (Fig. 3A) and P = 0.048 for ypT3 (Fig. 3B). On the other hand, when given a specific TRG (i.e., TRG2 or TRG3), the CSS of the patients was significantly different according to ypT stage (P = 0.047 for TRG2, Fig. 4A; and P = 0.035 for TRG3, Fig. 4B). However, in patients with ypN1-2 tumors, no similar significant association was found according to TRG or ypT stage.
DISCUSSION
Tumor response to preop-CRT spans a wide spectrum from the complete absence of viable cancer cells to no regression at all. In those who show favorable tumor responses, a higher rate of curative resection and a better chance to preserve adjacent pelvic organs and the anal sphincter are expected. Ultimately a higher local control rate and a higher disease-free survival rate are achieved. Previous studies reported that following preoperative CRT, respectability of over 80% was achieved, and complete pathologic response was observed in 10-20% [13-15].
For tumor response to preop-CRT, numerous factors are known to be influential [5, 16-18]. In the current study, these treatment-related factors, such as radiation dosage, use of chemotherapy, and interval between preop-CRT and surgery, were relatively homogenously controlled. However, the oncologic outcomes reported in the present study were poorer than those in previously published reports [19-21]. The interval between preop-CRT and surgery was relatively short (4-6 weeks in this study), and that might have influenced the outcomes. A long interval (6-8 weeks) between preop-CRT and surgery is known to be related with better tumor response and higher downstaging [18]. However, pCR rates were not found to be different in regard to the interval. Moreover, according to the report on long-term oncologic outcomes in the Lyon R09-1 trial, the interval was not found to be related to survival and local recurrence [22]. Thus, the poorer outcomes of the current study are more likely due to the advanced stages of the enrolled patients. We enrolled patients who showed fixed tumors on digital rectal examination and circumferential-margin-threatening or mesorectal-fascia-involving tumors on pelvic MRI.
Although tumor regression grade basically scores the ratio of residual cancer cell to radiation-induced fibrosis, a standard method for scoring tumor regression grade still does not exist. This is important because documentation of TRG can be different depending on the methods used to prepare slides, the number of slides reviewed per tumor, the experience of the reviewers, and so on. Mandard et al. [9] and other researchers [10, 23] advocated five-point grading systems while others [6, 7] advocated three-point systems. Ryan et al. [24] compared the five-point TRG and the three-point grade system with respect to tumor response after preoperative CRT for rectal cancer and evaluated both for intra- and inter-observer variability. They concluded that although prognostic impact might be the same, the three-point TRG was better with respect to intra- and inter-observer agreement. The three-point grade has the advantage of better reproducibility, with similar prognostic significance. Thus, we used the three-point grading system suggested by Rodel et al. [6].
Despite all the controversies, few studies performed subgroup analyses to shed light on the prognostic impact of TRG for specific group of the patients. As a whole, TRG has been uniformly found by univariate analysis to have a prognostic value for survival and recurrence in rectal cancer after irradiation [1, 3, 4, 6, 10, 25, 26]. Most series, however, have failed to establish TRG as an independent prognostic factor stronger than ypT or ypN [3, 4, 6, 10]. These results might indicate that the prognostic value of TRG was adversely impacted by stronger factors such as histopathologic N stage. In a large prospective series, Rodel et al. [6] found that in the analysis of a subgroup of patients with ypN0 tumors, the five-year DFS for patients with ypT3-4, ypN0 tumors showing intermediate tumor regression was superior to that for those showing poor regression. We demonstrated that for ypN0 patients, TRG was the most powerful prognostic factor, and this result supports that the finding of Rodel et al. [6]. On the basis of these results, we can assume that TRG has weak prognostic value in patients with lymph node metastasis, but that it has stronger prognostic value in patients without lymph node metastasis.
Wheeler et al. [7] postulated that although cancer invasion into the bowel wall progressed in a stepwise fashion, radiation therapy did not necessarily reverse those changes, but instead reduced the number of viable cancer cells (and normal cells) that were in the field of irradiation. They, thus, hypothesized that it would be appropriate to use a pathologic staging system that measured tumor regression of an irradiated rectal cancer in addition to the ypT and ypN stages because prognosis would differ according to both TRG and histopathologic stage. There have been many reports that indirectly support this hypothesis [3, 4, 6, 7]. In this study, we demonstrated no correlation between T-downstaging and TRG, which might reflect the quantitative fashion of tumor regression caused by preop-CRT. We found significant correlations of TRG with ypN stage and N-downstaging because both criteria are quantitative measures of metastatic lymph node involvement. With 4th or older versions of AJCC TNM systems, in which N stage was defined according to the anatomical location, such correlations might not have been found. We also observed different cancer-specific survivals according to different TRGs among the subgroups of patients with the same ypT stages. Thus, our conclusions support the suggestion by Wheeler et al. [7].
What happens if when we do not know about the lymph node status, for example, when a local excision is performed for a shrunk rectal cancer after preop-CRT? In that case, the possibility of lymph node metastasis should be carefully considered. Because of the low accuracy of lymph node evaluation when using conventional radiologic techniques, our question will be whether it is possible to predict lymph node metastasis based on clinical and histopathologic variables. In accordance with a previous study, our data showed a significant correlation of TRG with ypN stage and N-downstaging. However, our study showed that the percentage of patients with metastatic lymph nodes was as high as 11.7% for those who had shown complete regression (TRG1). We also observed that TRG1 (complete regression) and TRG2 (intermediate regression) showed a significant difference in the incidence of lymph node metastasis. According to Kim et al. [27], only complete regression was associated with a low incidence of lymph node metastasis, and a sharp demarcation existed between complete regression (2.2%) and nearly complete regression (16.1%). More recently, Caricato et al. [28] reported tumor regression in mesorectal lymph nodes of 35 rectal cancer patients treated with preoperative chemoradiation. They found an excellent correlation between lymph node regression grade and primary tumor regression grade; they also observed a sharp demarcation (11.7% vs. 45.6%) between complete regression and intermediate regression. Upon the basis of those results, we conclude that a good TRG still has a relatively high risk of lymph node metastasis and that although a correlation might exist between the responses of primary tumors and lymph node metastases, TRG is not an indicator for the response of lymph nodes, but is an indicator for the response of the primary tumor. Additionally, in contrast to previous literature [4, 25], our current recommendation is to perform standard radical surgery regardless of tumor response.
In this study, long-term oncologic outcomes in patients with rectal cancer who had been given preoperative chemoradiation therapy were found to depend on histopathologic T and N downstaging and on tumor regression grade. However, TRG alone may not be enough to give a prognosis. Thus, traditional histopathologic staging, especially N stage, remains the most important prognostic factor for cancer-specific survival, and TRG may aid in forming a prognosis for patients, particularly those without lymph node metastasis. In patients who achieved N-downstaging after preoperative chemoradiation, an accurate prediction of cancer-specific survival requires both information on the number of viable cancer cells remaining (TRG) and on whether the foci of viable cancer cells are located within or out of the rectal wall (ypT stage). Because not many prognostic factors are known for the patients without lymph node metastasis, the results of this study can be usefully applied to clinical practice.
According to the results from the current study, TRG following preop-CRT was found to have a limited prognostic significance for the treatment of locally advanced rectal cancer. Although as a whole TRG had a weaker prognostic power than ypN stage, it was found to have the strongest prognostic power in patients without lymph node metastasis. For better prediction of oncologic outcomes after preoperative chemoradiation therapy in locally advanced rectal cancer, tumor regression grade should be addressed in addition to the ypT and ypN staging system.