INTRODUCTION
A carcinosarcoma is a rare disease showing histologically malignant differentiation of epithelial and mesenchymal elements simultaneously, and its origin is still controversial [1, 2]. A carcinosarcoma may develop in many different organs, but most commonly it is found in the head and neck area and in the female reproductive organs. In the gastrointestinal system, a carcinosarcoma occurs in the esophagus, stomach and biliary duct primarily, and it has been rarely reported in the large intestine [1, 3-5]. Generally, a carcinosarcoma has an aggressive behavior and a poor prognosis. We report the case of a carcinosarcoma in the ascending colon, which was detected because of a bowel perforation.
CASE REPORT
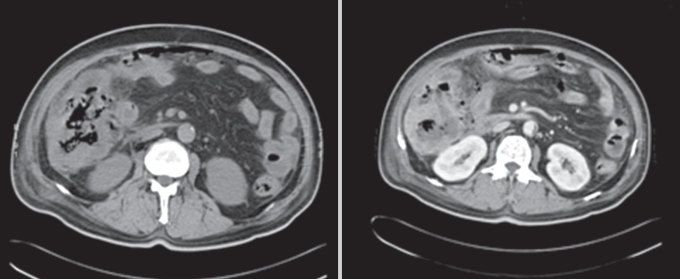
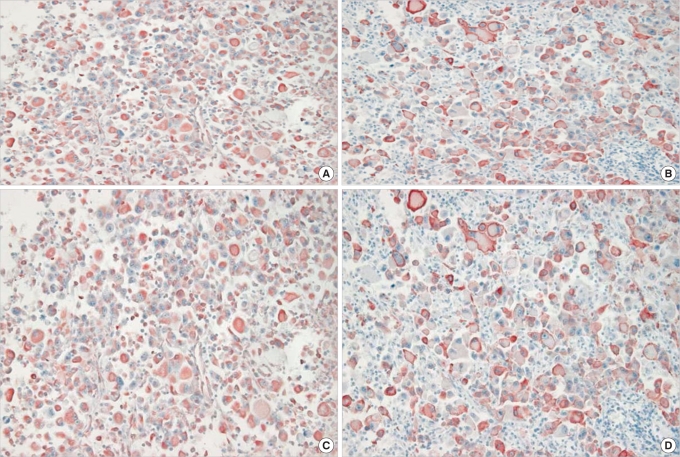
A 65-year-old male patient was admitted to the emergency room with chief complaints of abdominal pain and hyperglycemia that had lasted for one week. In the past history, he had hypertension and diabetes and was, thus, under medication. Regarding vital signs, his blood pressure was 150/80 mmHg, pulse rate was 100 times/minute, body temperature was 38.4Ōäā, and his heart sounds and lung sounds were normal. In the blood test, leukocytosis (white blood cell count, 12,900/mm3; hemoglobin, 12.0 g/dL; hematocrit, 36.2%; platelets, 242,000/mm3) was seen. In the blood chemistry, blood glucose was 536 mg/dL, and diabetic ketoacidosis was shown. On physical examination, direct tenderness and rebound tenderness were observed over the entire right abdomen. On computed tomography, pleural effusion and consolidation of both lungs were found, and ascending colon cancer with adjacent lymph node metastasis and infiltration to pericolic fat tissue accompanied by pneumoperitoneum were observed. The diagnosis was panperitonitis caused by perforation of the ascending colon cancer; thus, an emergency operation was performed (Fig. 1). In the surgical findings, contamination was severe, and a fungating round mass, 11 ├Ś 9 cm in size, with perforation was detected in the ascending colon and was located about 8 cm above the ileocecal valve; hence, a right hemicolectomy was performed. Although adhesion to adjacent tissues was severe, no distant metastasis or carcinomatosis findings were shown. On macroscopic examination, the mass was a gray, hard, round tumor with central ulceration, and in the cross section, invasion to pericolic fat tissue and several enlarged adjacent lymph nodes were observed. In the histological findings, most were poorly differentiated carcinomas, and sarcomatous and malignant fibrous histiocytomatous differentiation was detected together. Cancer cells penetrated the serosa and infiltrated to the pericolic fat tissue, and all were carcinomas histologically. On immunohistochemical staining, most carcinoma areas were strongly positive for cytokeratin, and the areas showing sarcomatous and malignant fibrous histiocytomatous differentiation were positive for cytokeratin and vimentin, but negative for desmin, which is a sarcoma marker (Fig. 2). Lymph node metastasis was detected in 11 of 13 lymph nodes.
The vital signs of the patient were stable after surgery, diet was initiated from postoperative day 5, and soft diet was taken without problems after postoperative day 8. Nevertheless, persistent leukocytosis was detected after postoperative day 16, and on computed tomography performed at that time, substantial ascites were detected. In paracentesis, cancer cells were detected; thus, carcinomatosis was suspected (Fig. 3). Afterward, the volume of ascites of the patient increased, and it could not be controlled. Pleural effusion also developed, and in thoracentesis, carcinomatosis findings were shown. The patient was transferred to the intensive care unit, and intensive treatments were administered; nevertheless, one month after surgery, the patient showed hematological instability and died of multiple organ failure.
DISCUSSION
A carcinosarcoma is a very rare disease, showing malignant differentiation of epithelial and mesenchymal elements simultaneously, and prognosis has been reported to be very poor. It occurs in the head and neck area, the respiratory system, and the female urogenital system most frequently. In the digestive system, its development in the stomach, biliary tract, and small intestine was reported in several studies. Nevertheless, its development in the large intestinal area is known to be very rare [1, 6, 7]. A carcinosarcoma in the large intestine was reported by Weidner et al. [1] in 1986 for the first time, and since Staroz et al. [8]. detected one in the descending colon in 1995, it has rarely been reported. Presently, including our case, 23 cases have been reported [1, 3, 4, 8-26] (Table 1).
The histological etiology of a carcinosarcoma has not been elucidated yet [1]. Until now, numerous hypotheses have been reported to explain the two histological characteristics of a carcinosarcoma. Recently, the hypothesis that precursor cells become cancer cells independently has been favored [2]. In addition, in studies that prove a histological conversion of the epithelium to the mesenchyme by detecting the presence of dysplasia and an adenocarcinoma in situ, a morphological transition area between carcinomatous and sarcomatous tissues was reported based on immunohistochemical staining [4]. It has been also proposed that the phenotype of the carcinoma is converted to a sarcoma due to a viral infection or a mutation of the p53 gene [9, 10].
Although the age was distributed primarily from 41 years to 84 years (average age, 68.36 years) in previous studies such as this case. In contrast to this case, the case of a 13-year-old girl was reported recently. In previous studies, carcinosarcomas are more prevalent in females and in the left large intestine [11, 27]. Prognostic factors are associated with the location of the carcinosarcoma, tumor size, depth of invasion, and clinical stage [2, 12, 28]. In regard to the location, the prognosis for a carcinosarcoma of the upper gastrointestinal tract is better than that for a carcinosarcoma of the lower gastrointestinal tract. Most carcinosarcomas develop in the upper gastrointestinal tract, including the esophagus and the stomach, and show a polyp differentiation pattern, and because of the characteristic of tumors growing rapidly to the lumen, the diagnosis is fast, so the prognosis is relatively good. On the other hand, symptoms of a carcinosarcoma in the lower gastrointestinal tract occur after development of distant metastasis in many cases; thus, diagnosis is difficult, and the prognosis is poor [4]. A carcinosarcoma is definitely diagnosed histologically, and it should show a sarcoma component and epithelial differentiation without showing a heterogenous mesenchymal component [3, 4].
Concerning clinical stages, the presence of distant metastasis is very important for prognosis. Regarding lymph node metastasis or distant metastasis, epithelial carcinoma factors are shown to be dominant over sarcoma factors [18]. The symptoms in our case were initiated by peritonitis caused by the perforation of the intestine, and the carcinosarcoma had progressed more rapidly due to the perforation. On the histological test, an undifferentiated carcinoma and sarcoma differentiation were observed together; nonetheless, the areas with cancer cells that had penetrated the serosa and had infiltrated into pericolic fat tissue were all carcinomas. Similarly, carcinoma components were detected in carcinomatosis that developed in the abdominal cavity and in the thoracic cavity after surgery.
Carcinosarcomas are treated similar to general colorectal cancer. Since prognosis is very poor, aggressive treatments and comprehensive follow-ups are required [12]. In regard to prognosis, because patients are not abundant, accurate data, such as 5-year survival rate, are absent. Nonetheless, according to studies reported in the literature, among the previously reported 22 cases, 12 cases died of the carcinosarcoma, and only one patient survived longer than five years [26]. Regarding its treatments, together with early diagnosis, radical resection is effective. In addition to surgical treatments, adjuvant therapies, chemotherapy (5-fluorouracil, leucovorin, doxorubicin and cisplatin) and radiation therapy have been attempted, but their effectiveness has not been proven yet [3, 4, 24].
A carcinosarcoma in the large intestine is a very rare disease, it shows malignant transformation of epithelial tissues and mesenchymal tissues, and its prognosis is poor because of rapid growth and metastasis to adjacent organs. Therefore, rapid imaging diagnosis and accurate pathological diagnosis should be made simultaneously. A radical resection over a wide area, considering local metastasis, distant metastasis, and invasion to adjacent organs, should be performed, and additional aggressive treatments, such as chemotherapy and comprehensive follow-ups, are required.