INTRODUCTION
Colorectal cancer is the third most frequently diagnosed cancer in both men and women and the second most fatal cancer [1]. The most important determinant of the prognosis in patients with nonmetastatic rectal cancer is mesenteric lymph node involvement. The presence of lymph node involvement allocates the rectal cancer patient to stage III according to the American Joint Committee on Cancer Staging System and the European Society for Medical Oncology [2, 3]. Guidelines suggest adjuvant chemotherapy and/or radiotherapy for N1 and N2 patients [4]. Although a lymph-node-negative tumor suggests a good prognosis, how the number of positive lymph nodes affects survival is a subject of debate. It has been suggested that at least 12 lymph nodes need to be removed within the specimen for accurate staging [5]. However, the National Comprehensive Cancer Network's (NCCN's) guideline for rectal cancer suggests preoperative chemotherapy and or radiotherapy for node positive patients. The NCCN proposes a postoperative adjuvant therapy for patients with medical contraindications to combined modality therapy [2]. Recent publications have suggested substantial variations in nodal staging attributable to surgical, pathological, and patient factors [6]. These clinicopathologic factors may affect the number of lymph nodes harvested during the surgical and/or pathological dissection. This may result in inaccurate staging and subsequent inappropriate therapy. However, some researchers believe that TNM staging may not be optimal and have proposed alternative lymph-node parameters [7].
The metastatic lymph node ratio (LNR) is defined as the ratio of metastatic lymph nodes to the number of total lymph nodes pathologically examined. This figure seems to be superior to the absolute number of metastatic lymph nodes in predicting the prognosis and to be useful in reducing stage migration in types of solid cancers such as cancers of the stomach [8-10], breast [11], bladder [12], pancreas [13], and lung [14]. Many clinical studies on colorectal cancer patients have been performed to investigate the significance of the LNR as a prognostic factor [13, 15-20]. However, the clinical significance of the LNR in rectal cancer patients' survival is still controversial. Some researchers found no correlation between the LNR and the survival rate [21] while others concluded that the LNR was a more critical prognostic factor than simple lymph-node metastasis [22]. Therefore, we aimed to investigate whether the LNR is a better prognostic factor than the absolute number of metastatic lymph nodes in cases of stage III rectal cancer. Also, we searched for a cutoff value of the LNR for predicting a prognosis for patients with rectal cancer.
METHODS
A retrospective review of a prospectively-collected database of rectal cancer patients operated on between March 2000 and December 2011 was performed to determine the effect of the LNR on disease-free survival (DFS) and overall survival (OS). A total of 228 patients underwent an operation due to rectal cancer, 85 of which were found to be in stage III. The study was basically conducted on stage III rectal cancer patients. All patients had received adjuvant chemotherapy. Patients who received neoadjuvant chemotherapy and/or radiotherapy and patients who did not receive adjuvant chemotherapy or radiotherapy were excluded. Fifty-five patients with stage III rectal cancer who fit these criteria were included in this study. All patients were staged preoperatively by using computed tomographic (CT) scans only. In some patients, magnetic resonance imaging or positron emission tomography-CT scan were added to preoperative evaluation, if needed. Parameters such as age, gender, type of surgery, preoperative careinoembryonal antigen (CEA) levels and adjuvant therapy were analyzed. Tumors were assessed for histological type, grade, stage, vascular invasion, lymphatic invasion and perineural invasion. The number of examined lymph nodes, the number of determined metastatic lymph nodes and the LNR were calculated for each patient. Recurrences and distant metastases were also documented.
All patients underwent a standard total mesorectal excision (TME) and a regional lymphadenectomy with tumor-free surgical and circumferential margins. High ligation was performed in all patients as a routine procedure at our clinic. Lymph nodes in the specimen were recovered by in vitro mesenteric dissection. Data on lymph node status were obtained from pathology reports. Tumors were staged according to the current American Joint Commission on Cancer (AJCC) TNM staging system. A combination of chemotherapy and radiotherapy was provided postoperatively to all patients. The postoperative adjuvant chemotherapy started within 2-4 weeks after the surgery and was given for 5 days every month by bolus infusing 5-fluorouracil and leucovorin six times. Radiotherapy began on the first day of the third cycle of intravenous chemotherapy, and fractionated irradiation of the whole pelvic cavity with a dose of 4,500-5,000 cGy was conducted.
Recurrence, whether loco-regional or distant, was confirmed histologically or clinically (palpable mass or tumor that may be associated with clinical deterioration identified on imaging studies and verified with increased serum CEA level). The survival analysis was performed using the Kaplan-Meier method. Cox regression analyses, after adjustment for potential confounders, were used to evaluate the relationship between the LNR and survival. A statistically significant difference was assumed if the P-value was less than 0.05.
RESULTS
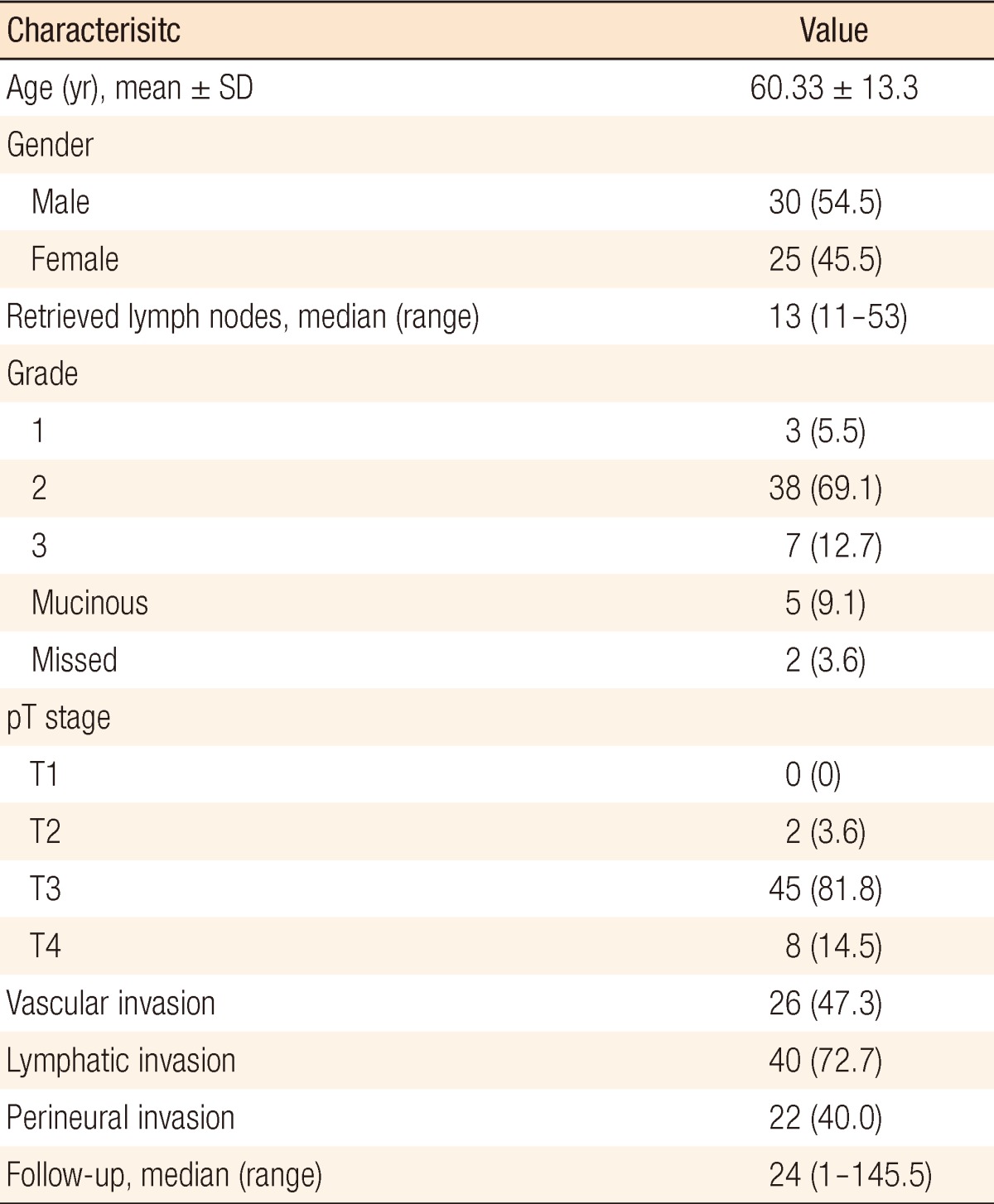
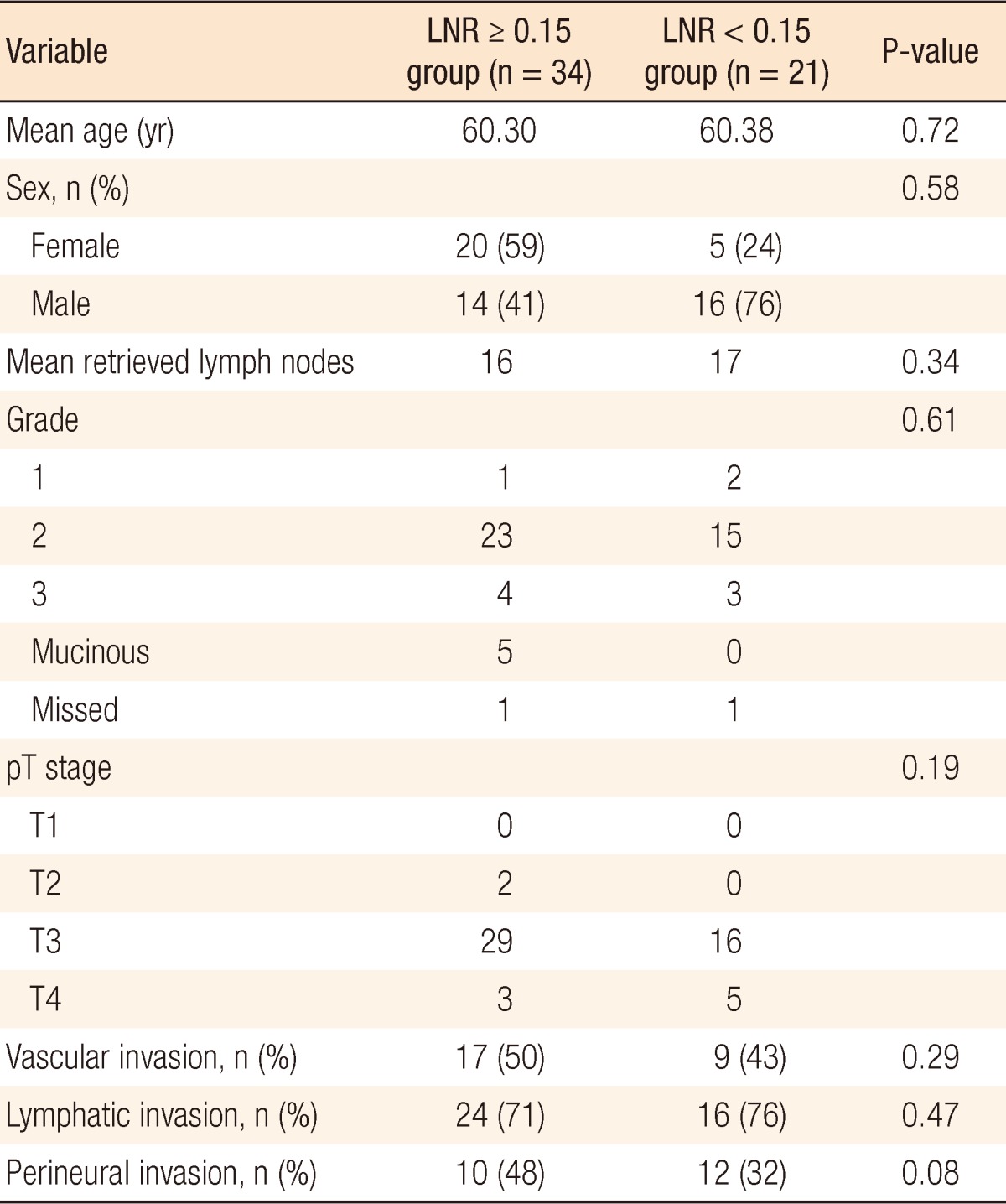
Fifty-five patients with stage III rectal cancer who underwent a curative resection were evaluated. Demographic data, histopathological characterisitcs, and tumor characteristics for patients are presented in Table 1. Tumor grades from pathology reports were unavailable for two patients. The mean age of the patients was 60.33 ┬▒ 13.3 years. Thirty (55%) were male and 25 (45%) were female. All patients were diagnosed as having an adenocarcinoma. The median follow-up for all patients was 24 months (range, 1 to 145 months). The median number of recovered lymph nodes was 13 (range, 12 to 53). An analysis of the data showed the median LNR value to be 23%. The study population was divided into 2 groups according to the LNR cutoff value of 23%. One group consisted of patients for whom the LNR was greater than or equal to 23% LNR. The second group consisted of patients for whom the LNR was lower than 23%. In Kaplan-Meier analysis, no significant difference was found between the 2 groups in terms of OS and DFS at the 1st, 2nd, 3rd, 4th, and 5th year after surgery.
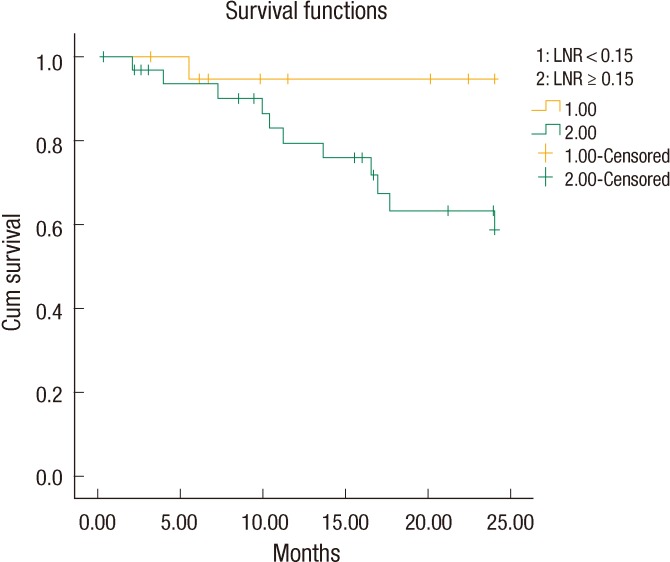
The LNR values lower than 23% were analyzed for each patient in descending order to find a cutoff value that resulted in a significant difference between the two groups. The OS and the DFS were compared between the two groups for each LNR value to find a cutoff value of the LNR that affected OS or DFS. Only for a LNR value of Ōēż15% was the two-year DFS significantly better than it was for patients with a LNR of greater than 15% (19.41 ┬▒ 1.3 months [67.6%] and 23.03 ┬▒ 0.9 months [95.2%], respectively, P = 0.02) (Fig. 1). When a multivariate Cox analysis for two-year DFS was done, we noted that none of the covariates affected the outcome (Table 2). Thus, the LNR 15% as a cutoff point was found to be an independent factor for predicting the two-year DFS in patients with stage III rectal cancer.
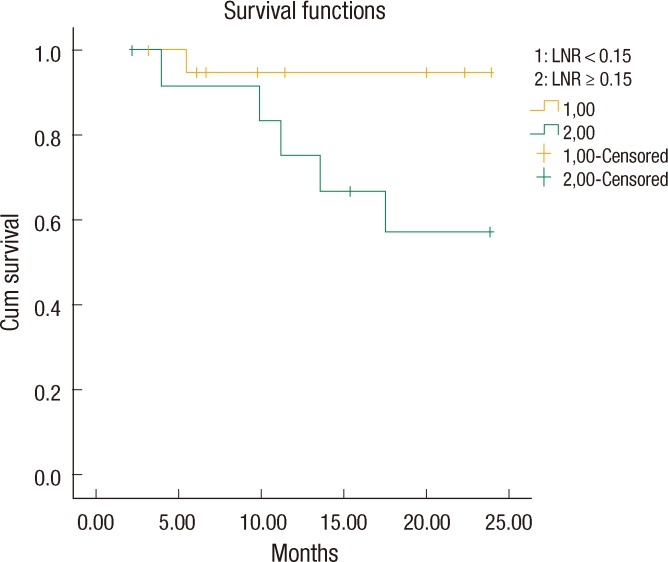
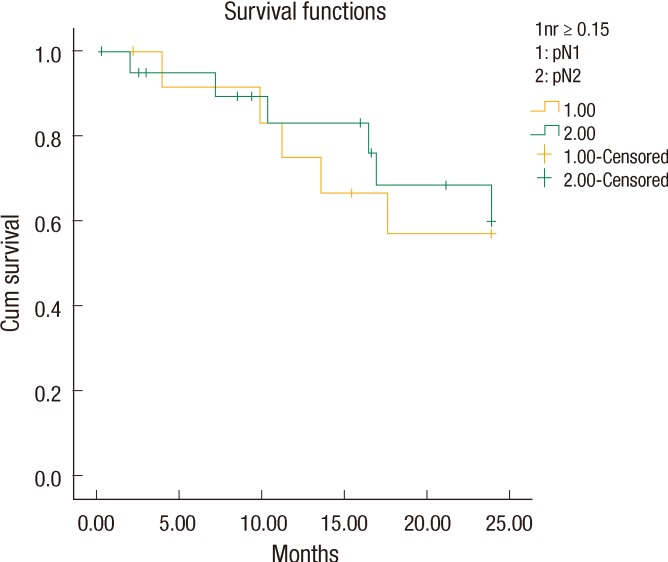
We noticed that all patients with LNR < 15% (n = 21) had a stage pN1 tumor, but the patients with LNR Ōēź 15% (n = 34) included both stage pN1 (13 patients) and pN2 (21 patients) tumors. We also found that the patients with a stage pN1 tumor and LNR Ōēź 15% had a two-year DFS of 61.5% (18.6 ┬▒ 1.9 months). However, the patients with a pN1 tumor and LNR < 15% had a better two-year DFS of 95.2% (23.0 ┬▒ 0.95 months, P = 0.023) (Fig. 2). Interestingly, the two-year DFS rate for LNR > 0.15 in patients with a pN1 tumor was not statistically significantly better than that for LNR > 0.15 in patients with a pN2 tumor (61.5% and 71.4%, respectively, P = 0.76) (Fig. 3).
DISCUSSION
Lymph-node metastasis is one of the most important prognostic factors in rectal cancer. Although the significance of number of retrieved lymph nodes has increased [23, 24], some have pointed out that the current N staging, which depends on the number of metastatic lymph nodes, does not reflect the prognosis accurately [25, 26]. Moreover, the number of retrieved lymph nodes is a variable that is affected by many factors including the individual characteristics of the patient, the competence of the surgeon, the ability of the pathologist to isolate and collect lymph nodes [27, 28], and the administration of neoadjuvant radiotherapy and/or chemotherapy [29]. Therefore, a better prognostic classification system is necessary to minimize the influence of the number of collected lymph nodes and to supplement the limitations of the current TNM system. This would also provide a more accurate disease staging, which would allow more appropriate adjuvant treatment planning and better calculation of the long-term prognosis for stage III colorectal cancer patients [30].
Because the survival rate for stage III rectal cancer varies widely [26, 29, 31], the clinical role of the LNR as a biologic predictor of prognosis has been demonstrated in some studies [18, 22, 32-35]. The present study investigated the LNR as a prognostic parameter for patients with stage III rectal cancer. Previous studies on the LNR for rectal cancer [33, 35, 36] determined cutoff values based on quartiles or complex statistical methods, so their results were difficult to apply in daily clinical practice. That is the reason we tried to identify a single cutoff value for the prognostic stratification by dividing all patients into two groups according to a certain LNR value. Unlike patients with colon cancer, patients with rectal cancers are routinely considered for neoadjuvant chemo/radiotherapy before undergoing surgical resection. Besides shrinking the primary tumor and reducing the risk of local recurrence after surgery, radiotherapy may also decrease the number of local lymph nodes [37]. As a consequence this may decrease the number of lymph nodes retrieved, which may negatively affect the LNR values. Because of that, in this study, we did not include patients who had received neoadjuvant chemo/radiotherapy; thus, we were able to achieve more accurate ratio-based staging.
Reasons for not administering neoadjuvant chemo/radiotherapy in our study group were unavailability of radiotherapy, preoperative mis-staging, patient's refusal, and surgeon's preference. This made our study population distinctive. All the patients included in this study were operated on by using the TME technique and received adjuvant chemo/radiotherapy after surgery. Schumacher et al. [16] identified a LNR of 8% as a breakpoint for predicting the five-year OS and DFS in all stages of colon cancer. The survival analysis of stage III colon cancer patients revealed that a LNR of 18% was predictive of the five-year DFS [15]. Our study investigated the predictive value of the metastatic LNR for stage III rectal cancer, not colon cancer. No significant difference was detected between our two groups in terms of the OS and the DSF at the 5th, 4th, and 3rd years after surgery. This may be due to the limited number of patients in our study and the limited follow-up period. However, we found that a LNR of 15% was a cutoff point for predicting the two-year DFS. Because over 80% of recurrences in colorectal cancer usually occur in the first 2 years following surgery [38], we can conclude that our results show that the LNR has a good predictive value for recurrence of rectal cancer. Dekker et al. [36] showed that in addition to the 7th edition of the Union for International Cancer Control/AJCC TNM classification, the metastatic LNR was an independent prognostic factor for OS and local recurrence in stage III rectal cancer. In our study, the multivariate Cox analysis showed that the LNR was an independent prognostic factor for DFS in stage III rectal cancer. The metastatic LNR has been reported to be a better prognostic factor for survival in stage III rectal cancer than the currently-used lymph-node staging method in the TNM system [18, 32, 34]. A few studies recently investigated the LNR in rectal cancer and reported a significant correlation between the LNR and survival [22, 33, 35, 39, 40]. However, previous studies on the LNR in rectal cancer selected cutoff points arbitrarily [35]. We simply found a single LNR cutoff point in rectal cancer, which differentiates our study from other studies.
Our study differs from others investigating the LNR in that it used a single cutoff value for a comparison of higher and lower values. Previous studies were also different from this study in that they compared the prognostic values of the LNR and N staging by separating them into many groups, which produced unclear results [33, 35]. We divided our patients into two groups. In addition, previous studies included all rectal cancer patients, even those having neoadjuvant therapy, in the analysis. We did not include this group of patients so as not to affect the number of metastatic lymph nodes. We found that all patients with LNR < 15% (n = 21) had a stage pN1 tumor, but contrary to our expectation, patients with LNR Ōēź 15% (n = 34) consisted of those with stage pN1 and pN2 tumors (N1, 13 patients; N2, 21 patients). We also found that patients with a stage pN1 tumor and LNR Ōēź 15% had a two-year DFS of 61.5% (18.6 ┬▒ 1.9 months). However, the patients with a pN1 tumor and LNR < 15% had a better two-year DFS of 95.2% (23.0 ┬▒ 0.95 months, P = 0.023) (Fig. 2). The two-year DFS in LNR Ōēź 15% patients with a pN1 tumor was not significantly better than that in LNR Ōēź 15% patients with a pN2 tumor (61.5% and 71.4%, respectively, P = 0.76). This result supports reports that show the LNR to be a more accurate prognostic factor for survival in stage III rectal cancer than the currently-used lymph-node staging method in the TNM system. Similar results were shown by Park et al. [41] who showed that the five-year survival rates differed with the LNR in patients with N1-stage cancer. They also suggested that the five-year survival rates of the patients with N2-stage cancer were not different for a LNR with a cutoff of 7%. Inoue et al. [9] and Bando et al. [10] insisted that the LNR was more meaningful for giving a prognosis because it reduced stage migration. These findings suggest that the LNR can replace N staging and that a revision of the current TNM staging is needed. Determination of the optimal approach to quantify the lymph-node status in colorectal cancer will help accurate patient staging, allow appropriate adjuvant treatment planning, and provide a better prediction of the long-term prognosis. This study supports recent studies showing that the LNR correlated with the prognosis.
In conclusion, our study showed the prognostic significance of a ratio-based staging system for rectal cancer. This may help in developing more accurate staging systems. In addition, we demonstrated that a ratio of 15% represents the LNR cutoff point for predicting a prognosis for patients with rectal cancer.