Treatment Strategy for Perianal Fistulas in Crohn Disease Patients: The Surgeon’s Point of View
Article information

Abstract
Perianal fistula is a frequent complication and one of the subclassifications of Crohn disease (CD). It is the most commonly observed symptomatic condition by colorectal surgeons. Accurately classifying a perianal fistula is the initial step in its management in CD patients. Surgical management is selected based on the type of perianal fistula and the presence of rectal inflammation; it includes fistulotomy, fistulectomy, seton procedure, fistula plug insertion, video-assisted ablation of the fistulous tract, stem cell therapy, and proctectomy with stoma creation. Perianal fistulas are also managed medically, such as antibiotics, immunomodulators, and biologics including anti-tumor necrosis factor-alpha agents. The current standard treatment of choice for perianal fistula in CD patients is the multidisciplinary approach combining surgical and medical management; however, the rate of long-term remission is low and is reported to be 50% at most. Therefore, the optimum management strategy for perianal fistulas associated with CD remains controversial. Currently, the goal of management for CD-related perianal fistulas are controlling symptoms and maintaining long-term anal function without proctectomy, while monitoring progression to anorectal carcinoma. This review evaluates perianal fistula in CD patients and determines the optimal surgical management strategy based on recent evidence.
INTRODUCTION
Perianal fistula is an abnormal connection between the anorectum and perianal epithelium [1]. Perianal fistulas are frequently observed in Crohn disease (CD) patients and are the most common symptom in CD patients seen by colorectal surgeons [2]. Presence of anorectal stricture, male, perianal abscess, and rectal inflammation are associated with perianal fistula related to CD [3]. The cumulative incidence of perianal fistulas among CD patients in the US is approximately 10% at 1 year after diagnosis, 15% at 5 years, 18% at 10 years, 23% at 20 years, and 24% at 30 years [2, 4]. The overall prevalence of perianal fistulas in Europe, estimated as the sum of the estimated prevalence for all etiologies, was 1.69/10,000 population [5]. In a multicenter study in Korea, 35% of CD patients had a history of perianal fistula, while 28% had concomitant perianal fistulas at the time of the CD diagnosis [6, 7].
In the Montreal revision of the Vienna classification, the 3 predominant parameters of age at diagnosis, location, and behavior were not changed, but perianal disease alone required separate subclassification [8]. There are substantial data that perianal disease is not necessarily associated with intestinal fistulizing disease [9]. Although perianal fistula is not associated with the locationbased classification, the risk of perianal fistulas is up to 92% higher in those with colonic disease with rectal involvement [2].
The presence of perianal fistula negatively affects a patient’s quality of life due to the occurrence of pain, perianal discharge, and the impairment of both physical and sexual functions [10]. The treatment goal of perianal fistula in CD is the resolution of the perianal fistula, improvement of quality of life, maintenance of fecal continence, and avoidance of proctectomy with stoma creation [11].
Currently, the best approach to achieve the resolution of perianal fistula is a combination of medical and surgical management, resulting in fistula healing in 50% of patients [10, 12]. The improvement in biologics and management strategy, i.e., top-down treatment, have led to a rise in the rate of complete remission in the treatment of CD, but the rate of perianal fistula healing remains low [13]. Recent reviews are mainly related to medical treatment, but the effectiveness of new biologic agents requires further evaluation.
The aim of the current review was to demonstrate the evidence regarding surgical treatment of perianal fistulas in CD patients and to discuss in detail multidisciplinary surgical treatment strategy.
CLASSIFICATION, OUTCOME EVALUATION, PROGNOSTIC FACTORS
Classification of perianal fistulas in Crohn disease patients
Surgical treatment of perianal fistula can vary from simple abscess drainage to a surgical approach depending on the type and the extent of the fistula. Therefore, anatomical description with appropriate classification of the perianal fistula is crucial before starting any kind of management (medical or surgical). The anatomical description of fistulas should include the type of fistula, location of internal and external openings, and the presence of secondary branches and abscesses. There are several classifications of perianal fistulas, from the oldest Goligher classification to the recent American Gastroenterological Association (AGA) classification. A clinically useful classification of perianal fistulas in CD should enable the physicians to determine the optimal management strategy; however, there is no consensus regarding which classification system should be used. Therefore, many studies classify the type of anal fistula in CD patients as ‘mixed.’ The current review analyzes the types of perianal fistula in CD patients, a factor contributing to the selection of the management strategy.
The traditional classifications include those proposed by Goligher (1875), Milligan-Morgan (1934), Parks (1976), and Eisenhammer (1978), especially for horseshoe fistula [14]. The traditional classification widely used to date is the Parks classification, which was a result of an analysis of 400 patients [15] and provided a detailed description of the course of the perianal fistulous tract in relation to the external and the levator ani muscle. However, this classification does not provide any information regarding the complexity of the fistula (secondary tracts or the presence of abscess) or the presence of proctitis [3]. The Parks classification is considered to determine the type of usual perianal fistula, but perianal fistula arising from CD is more complicated. The AGA classification (2003) proposed that perianal fistulas should be divided into 2 categories based on fistula tract anatomy, the number of external openings, and presence of abscess and/or proctitis; simple or complex [16]. This classification has prognostic relevance for fistula healing as patients with more complex fistula are less likely to achieve clinical remission than patients with simple fistulas [17]. However, the “complex fistula” category is based on multiple variables and does not permit proper individualization of treatment [3]. The St. James University Hospital (SJUH) classification (1996) [18, 19], based on magnetic resonance image (MRI) findings, has 5 grades based on detailed information on the primary fistulous tract, its relation to the sphincter, and on secondary tracts and related abscess [19]. This classification enables objective preoperative assessment for the colorectal surgeon and is more predictive of surgical outcome than preoperative or intraoperative classification [20]. However, this classification is not simple to apply in daily clinical practice. The Hughes-Cardiff classification (1978) [21], which is less commonly used, divided fistulas into simple and complex categories and had advantages in terms of prognostic value but lacks information on anatomical description (Table 1).

Classification of type of perianal fistula
How to determine the remission status and drainage status of perianal fistulas?
To describe the outcomes, the remission status needs to be defined. Complete remission is defined as symptomatic and radiographic remission; symptomatic remission, the absence of both pain and drainage from the fistula tract; and radiographic remission, the absence of inflammation in any fistula tract and the absence of any abscess based on the Toronto consensus [22]. Furthermore, symptomatic response is defined as meaningful improvement in the symptoms of pain and drainage as judged by both the patient and physician in the absence of remission; this response should not be considered a desirable final outcome but is useful to assess early response to treatments [22]. From the radiologic point of view, deep remission is defined as the presence of clinical remission and the abscess of anal canal ulcers and fistula healing on MRI [23]. The timing of evaluation of remission or response is reported differently for each study results from 8 weeks to 12 months [22, 24-26].
To evaluate the efficacy of management, a clinical trial used a simple fistula drainage assessment that defined “closure” when a fistula no longer showed drainage despite gentle finger compression; “response,” a reduction of 50% or more in the number of draining fistulas on at least 2 consecutive visits; and “remission,” the absence of any draining fistulas on 2 consecutive visits [27]. The “gentle finger compression” approach is largely investigator dependent and has never been formally validated [28]. The presence of a persistent tract without fluid drainage is defined as “remission.” The external appearance of the fistula is used as a surrogate for the whole internal fistula tract [28]. MRI studies have shown that internal fistula healing lags behind clinical remission by a median of 12 months.
Prognostic factors for recurrence and poor healing
Understanding the risk factors for recurrence helps colorectal surgeons and patients in the optimal management of a perianal fistula in the context of CD. Generally, perianal fistulas healed better and the recurrence rate was lower in patients without rectal involvement than in those with rectal involvement [29]. It has been reported that the need for proctectomy is significantly higher in patients with rectal involvement [25, 30, 31]. Therefore, rectal involvement of CD is considered a poor prognostic factor. Besides, the complex type of perianal fistulas also showed lower remission rates and higher recurrence rates; it can be considered a prognostic factor [29, 31-33]. However, since the definition of a complex fistula was slightly different in each study, it is necessary to properly define it in the future.
A meta-analysis using the data from 6,168 patients (20 eligible studies) reported risk factors for anal fistula recurrence, divided into patient-related factors and surgery-related factors [34]. The pooled recurrence rate from this meta-analysis was 19%, which ranged from 2.5% to 57.1% [34]. Prior anal surgery showed a significant association with anal fistula recurrence and surgery in terms of patient-related factors [34]. Although smoking was previously known as a risk factor for recurrence [35, 36], this metaanalysis reported that there was no correlation between smoking and recurrence [34]. Besides, in terms of poor healing, rectovaginal fistula and the nucleotide-binding oligomerization domain 2 (NOD2) variant were related to a lower probability of complete remission and a longer time to complete fistula closure [37-39]. In clinical practice, NOD2, the first CD gene identified, represents the strongest genetic predictor of CD susceptibility and phenotype and the NOD2 variant is strongly associated with the development of perianal fistulas [38]. In the era of biologic treatment, the presence of CD granulomas in the perineum reduced the chance of healing or improvement of a perianal fistula [40].
In terms of surgery-related factors, a high transsphincteric fistula, an unidentified internal opening, horseshoe extension, and multiple fistulas were significantly associated with recurrence after surgery [34, 41-46]. In a meta-analysis regarding surgery, there was a significant difference in recurrence prognostic between seton procedure and fistulotomy (relative risk, 2.97; 95% confidence interval, 1.43–2.59), but recurrence prognosis was not different between fistulotomy and fistulectomy and between use of endorectal mucosal advancement flap (EMAF) and fistulotomy [34, 41, 42, 47, 48].
MANAGEMENT STRATEGY
Colorectal surgeons should carefully examine the perianal fistula and review the preoperative imaging, such as 3-dimensional endorectal ultrasound (EUS), computed tomography (CT), and MRI images, to understand the anatomy of the perianal fistula and obtain exact prognostic information. Prior anal surgery is a poor prognostic factor for recurrence [34, 45]; therefore, the first surgery is the best chance to obtain complete remission. The decision to perform surgical treatment for perianal fistulas in CD patients must be individualized and based on the extent of disease and severity of symptoms. Despite the best available medical and surgical management strategies, perianal fistula in CD patients have a poor prognosis and may result in the need for proctectomy or permanent diversion in some patients with severe perianal fistula [49-54]. A consensus described the goals of treating perianal fistulas, with the short-term goals as abscess drainage and reduction in symptom severity and the long-term goals as the resolution of fistula discharge, improvement in quality of life, fistula healing, resolution of fecal incontinence, and avoiding proctectomy with stoma creation [11]. Therefore, the current review discusses management strategy based on the presence of symptoms, extent of disease, and management goals.
Simple, asymptomatic perianal fistula without rectal involvement of Crohn disease
There have been few studies or recommendations about simple, asymptomatic perianal fistulas related to CD. The American Society of Colon and Rectal Surgeon (ASCRS) recommends that patients with asymptomatic anal fistulas which are accidentally discovered with no signs of local sepsis require no surgical intervention [55]. The second Korean guidelines for the management of CD also recommended that this type of perianal fistulas do not require treatment [56]. These fistulas may remain indolent for an extended period of time; therefore, patients need not be subjected to the morbidity of operative intervention (Table 2 [3, 10, 22, 54-56]). Considering that antibiotics improve fistula symptoms but do not induce fistula closure [57, 58], these patients do not need antibiotic therapy. Even if no management is required for this type of perianal fistula, exam under anesthesia (EUA) by colorectal surgeon; imaging studies including EUS, CT, or MRI; and endoscopy to evaluate the rectal involvement in the presence of CD are needed to ensure accurate fistula diagnosis and classification.
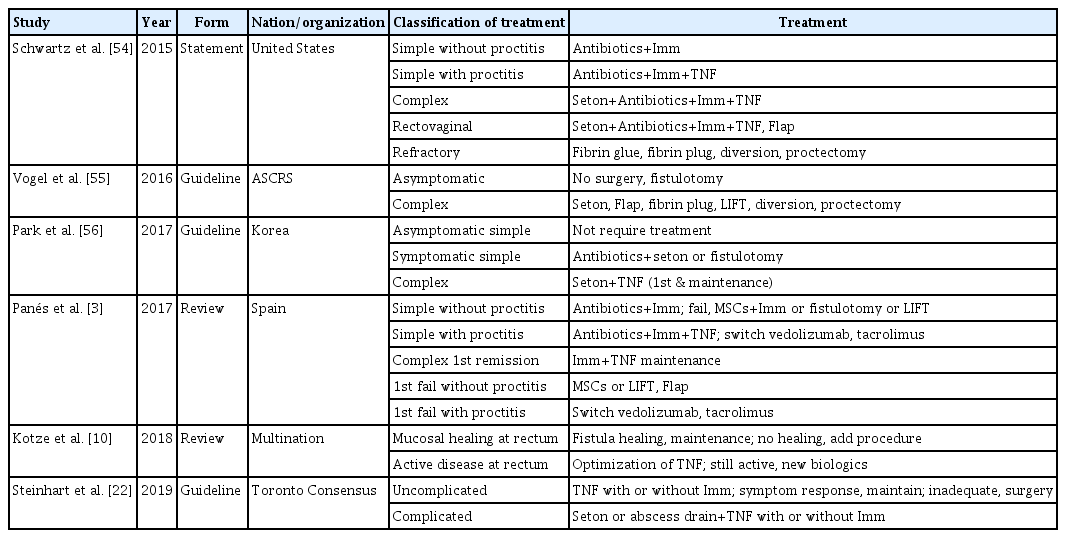
Treatment strategy of the recent guidelines or reviews
Simple, symptomatic perianal fistula without rectal involvement of Crohn disease
Surgical or medical treatment should be considered for simple, symptomatic perianal fistulas in CD patients [55, 56]. A natural history study found that more than 70% of patients achieved complete remission after undergoing medical or surgical treatment [32]. If the patients developed superficial or ischiorectal abscesses, these abscesses should be drained externally by incision and drainage for relieving symptoms, followed by EUA [59, 60]. Antibiotics, most commonly ciprofloxacin and metronidazole, are considered the first-line treatment for this type of fistula. Evidence on the use of antibiotics is limited and comes from small case series. Studies on metronidazole or comparing the efficacy of ciprofloxacin and metronidazole have shown that patients responded to antibiotics, but complete remission was difficult to achieve with antibiotics [57, 58].
An old, retrospective, surgical case series on this type of fistula has shown that fistulotomy alone induced remission in 85% of patients with this type of fistula [61]. Other studies also reported that 62%–100% of patients achieved complete remission after fistulotomy with a mild incontinence rate of 6%–12% [62-66]. Ligation of intersphincteric fistula tract (LIFT), first described in 2007, may be also considered for this type of fistula [67, 68]. The rate of perianal fistula healing following LIFT ranges from 48% to 67% depending on the duration of follow-up without reported incontinence [69]. A small case series prospectively evaluated 15 patients with CD undergoing LIFT for transphincteric fistulas and found improvements in the Wexner Perianal Crohn’s Disease Activity Index (PCDAI) and McMaster PCDAI from 14.0 to 3.8 and 10.4 to 1.8, respectively [70]. The rate of perianal fistula healing following EMAF ranges from 33% to 93%, but incontinence is reported in approximately 10% of patients, and this proportion may be higher in the presence of scarring due to a prior attempt of fistula repair [71]. Although the evidence was limited and the number of cases was small, fistulotomy or LIFT alone was recommended for the management of this type of perianal fistula (Table 2). Before starting or continuing medical treatment, waiting for symptomatic relief and resolution of skin erythema is required.
Complex perianal fistula in Crohn disease patients
Complex perianal fistulas are estimated to account for 70% to 80% of perianal fistula in CD patients, as defined by the AGA classification [72]. These fistulas have a high location of origin from the fistulous tract, multiple external openings, are associated with pain or fluctuation (abscess), and/or are connected to an adjacent structure (bladder, vagina) [16]. Ultimately, 10% to 20% of CD patients with perianal fistulas require proctectomy or proctocolectomy, with up to 25% of these patients experiencing poor wound healing or the formation of a perineal sinus as a surgical complication [3]; therefore, careful and strategic management is required for complex perianal fistulas in CD patients.
Seton procedures are a common practice in the management of perianal fistula in CD patients [73]. Seton procedures are used to drain the fistula and prevent the accumulation of pus, which may lead to recurrent abscesses, and minimize sphincter injuries in an attempt to closure of the fistula tract. Seton procedures involve surgical thread loops passed from the internal to the external opening of the fistula tract and exteriorized through the anorectal canal [74]. In patients about to start biologic therapy, colorectal surgeons aim to provide a fully drained the complex perianal fistula to reduce the risk of abscess formation and to improve the likelihood of success with medical treatment [75]. The recent European Crohn’s and Colitis Orgarnisation (ECCO) guideline states that the key surgery of the complex perianal fistula is controlling perianal sepsis by EUA and appropriate seton procedure [76].
Physicians have utilized this function of seton procedures but are aware of the concern that epithelization may occur if the healing timing of perianal fistula is left too long, and this may hinder the response to medical or surgical treatment. Based on the findings of a randomized controlled trial (Treatment of Perianal Fistulas in Crohn’s Disease, Seton Versus Anti-TNF Versus Surgical Closure Following Anti-TNF [PISA] study), chronic seton placement should not be recommended as the sole treatment for perianal fistulas in CD patients [77, 78]. Although there are no guidelines for the timing of removal, seton drains may be retained in the long-term (months to years) without negative consequences depending on clinical scenario and patient factors, but leaving seton in place may interfere with the wound healing of fistula track itself. A study on the timing of seton removal should be conducted. Cutting seton drains are generally not recommended due to the risk of damage to the sphincter and deformation of the anus [79].
Seton procedures have a low incidence of re-intervention, recurrent abscess formation, and side-branching of the fistulous tract, with preservation of this fistulous tract’s patency and cost-effectiveness [80]. The major disadvantages of seton procedures are discomfort and time to achieve stability. The major disadvantage associated with anti-tumor necrosis factor-alpha (anti-TNF-α) therapy as the sole therapy includes a high re-intervention rate, prolonged maintenance therapy, high recurrence rate, and severe side effects. Therefore, seton procedures and anti-TNF-α therapy should be used concurrently to increase the fistula healing or closure rate. Overall, combined medical and surgical management with drainage, seton procedures, and infliximab therapy has been shown to be superior to either medical or surgical treatment alone [56, 78].
Recurrent or persistent perianal fistula in Crohn disease without rectal involvement
Use of EMAF is a reasonable approach to treating recurrent or persistent perianal fistulas in the absence of proctitis or stenosis [81]. A major advantage of this procedure is that it avoids external wounds that are difficult to heal. In CD patients, the pooled success rate of EMAF is approximately 66% [40, 82], and a recent meta-analysis observed a 61% success rate [83]. However, surgeons should be careful about the higher rate (7.8%) of fecal incontinence after EMAF, compared with the rate of LIFT (1.6%) [83]. Patients with a failed initial flap procedure are candidates for a repeat procedure, although failure rates expectedly increase with repeat attempts [84]. Healing rates have improved over time, as patients are treated with biologic therapy, video-assisted anal fistula treatment (VAAFT), and platelet-rich plasma adjuncts [82, 85, 86]. Anal fistula plugs and fibrin glue have both been studied in CD patients with low rate of complete healing, especially for recurrent or persistent perianal fistula in CD patients; therefore, both techniques should be considered carefully when used to resolve this type of perianal fistula [87-89]. A systematic review showed that the pooled success rate of plugs for the recurrent perianal fistula was 40% [90]. Fibrin glue showed a wide range of success rates with limited efficacy [76], rather, fibrin glue is being used in combination with stem cell therapy and reported good results [91].
An area of emerging research is the injection of stem cells into fistula tracts. The phase III randomized controlled ADMIRE-CD (Adipose Derived Mesenchymal Stem Cells for Induction of Remission in Perianal Fistulizing Crohn’s Disease) trial found that injection of allogeneic expanded adipose-derived stem cells directly into treatment-refractory complex perianal fistulas of 212 patients with CD resulted in remission in 51.5% of patients at 24 weeks and 56.3% of patients at 52 weeks, compared to a remission rate of 35.6% at 24 weeks and 38.6% at 52 weeks with saline placebo [72, 92]. A phase II trial reported that long-term results of autologous adipose-derived stem cell therapy were 75% complete healing at 24 months [93], and this trial is conducting a phase III clinical study in CD patients with complex and recurrent perianal fistulas. More recently, a phase-I trial studied the application of mesenchymal stem cells-coated fistula plugs into 12 patients with chronic perianal fistulas and showed 83% complete clinical healing at 6 months [94]. Although there are no studies comparing autologous and allogeneic stem cells for perianal fistula [76], stem cell therapy could be an effective and safe treatment option for perianal fistula in CD (Table 3 [32, 58, 70, 72, 88, 92-107]).

Results from the recent prospective studies
Perianal fistula in Crohn disease patients with horseshoe abscesses
Deep postanal abscesses comprise less than 15% of all types of anorectal abscesses [108]. For the treatment of deep postanal abscesses with unilateral or bilateral horseshoe extensions, the modified Hanley procedure is recommended [109]. After a full debridement of any abscesses, a silastic drain may be passed from the posterior incision through the lateral incisions on both affected sides and when present the fistula can be controlled with a draining seton. When the abscess is controlled and the erythematous skin is subsided, the management should be performed according to the management strategy of the complex perianal fistula.
Refractory or uncontrolled perianal fistula in Crohn disease (diversion/proctectomy)
Patients with refractory perianal disease may require temporary fecal diversion or proctectomy. A meta-analysis of 16 studies including 556 patients for refractory perianal CD reported an early response in 63.8% of patients and low attempts (34.5%) and low success rate (16.6%) of restoration of bowel continuity after fecal diversion, and finally, 41.6% of patients who failed temporary diversion required proctectomy [110]. Proctectomy is the last option for refractory or uncontrolled perianal fistula in CD patients that has not responded to both aggressive medical and surgical management. Although rectal involvement is associated with a higher rate of proctectomy compared with rectal sparing (29%–77% vs. 4%–13%) [31, 65], rectal involvement alone could not determine proctectomy and fecal diversion might offer an alternative to extensive resection [111]. In cases with concomitant Crohn colitis and perineal disease, proctocolectomy is preferred over rectal preservation due to the high incidence of persistent rectal stump disease when a stump is left in situ [112]. In terms of poor wound healing or a persistent perineal sinus after proctectomy or proctocolectomy, risk factors associated with a persistent sinus are younger patient age, fecal contamination, and extrasphincteric dissection, needed in cases of severe anorectal disease [113]. When deciding on a proctectomy, these results should be fully considered and explained to the patients. The patients who have had perianal fistulas for more than 10 years are likely to be associated with cancer [114], therefore, patients with long-standing refractory perianal fistulas should be monitored carefully for cancer.
SURGEONS’ PERSPECTIVES
Perianal fistulas are generally classified into 2 types in the clinical setting based on the AGA classification; simple and complex. However, in the case of high fistulas, the definition of “high” should be accurately established, e.g. trans-, supra-, and extrasphincteric fistulas. The use of antibiotics is likely to be decided depending on the patients’ condition as mentioned in the current review, but studies on the use of antibiotics during the follow-up period or clinical course according to different situations are insufficient. Although the seton procedure is the most widely used and known as one of the most appropriate surgical methods, further research on the appropriate timing of seton removal will be needed. From the point of view of the colorectal surgeon, the timing of referring to medical treatment after surgery is important, and it is necessary to study when the escalation of drug dose or the change of kind of drug should be started after surgery [115]. The timing of outcome assessment varies in each study, from 8 weeks to 12 months after surgery. Therefore, physicians should evaluate the schedule and intervals between testing to determine outcomes.
CONCLUSIONS
To plan the management of a perianal fistula in CD patients, thorough examination of the perianal fistula and risk evaluation are required. Asymptomatic perianal fistula in CD patients without rectal involvement do not need interventions. After controlling symptomatic lesions, perianal fistulas should be managed using combined medical and surgical treatment for achieving complete remission. Surgical treatment of a simple, symptomatic perianal fistula without rectal involvement mostly involves fistulotomy with the short-term use of antibiotics and in recent cases, LIFT. Complex perianal fistula treatment should be microinvasive, involving non-cutting seton procedure, followed by medical treatment. For persistent and refractory perianal fistula, use of EMAF, anal fistula plug, fibrin glue, and VAAFT have been used, but the rate of complete remission is not promising. Some stem cell studies for complex, recurrent, and persistent perianal fistula showed good results, but in order to actively introduce stem cell therapy, long-term results and more clinical phase III study results will be required. Diversion or proctectomy is the final stage in the treatment of perianal CD in the patient with severe and long-standing perianal fistulas with malignancy concerns.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.