INTRODUCTION
The COVID-19 pandemic crisis has had a staggering impact worldwide. Confirmed cases have increased exponentially and the number of infected individuals has since exceeded a million [1]. It is however important to realize that with limitations in testing, true infection rates may in fact be much higher [2]. In addition, presymptomatic transmission of infected individuals has been documented in China and lately confirmed in Singapore [3-5]. Our local data suggests that this can occur in 6.4% of patients but has been reported to be as high as 30% in other studies [6,7].
Safe surgery has emerged as a topic of immense interest. As colorectal surgery accounts for a significant proportion of General Surgery workload [8], the COVID-19 pandemic thus has immense implications for many general and colorectal surgeons. In this current juncture of the pandemic with dangers of viral transmission, surgeons need to achieve a balance between surgical safety and judicious consumption of personal protective equipment (PPE). While deferment of nonurgent cases may be an initial strategy, this approach is impractical in the long run. The COVID-19 pandemic will likely have a protracted course and the resultant backlog of cases from indiscriminate deferment may overwhelm surgical capacity in the near future and compromise clinical care [9]. This is particular pertinent for common and time-sensitive pathologies like colorectal cancer.
In Singapore, COVID-19 management has been one of prompt contact tracing and isolation to prevent transmission. Curtailment of travel as well as safe distancing measures at work and social areas have all been imposed. Nonetheless, there have been a large number of imported cases with resultant community spread. In the authorsŌĆÖ hospital, there have been 290 (latest figures as of 23/4/20) positive COVIDs to date.
While there has been a gradual reduction of elective workload over the last 2 months since the onset of the disease outbreak in Singapore, there continues to be a reasonable volume of cases performed. In this article, we share our colorectal unitŌĆÖs workflow (Fig. 1) and recommendations (Table 1) for safe practice in the COVID-19 era.
Workflow for patients undergoing elective colorectal procedures in the COVID-19 era:
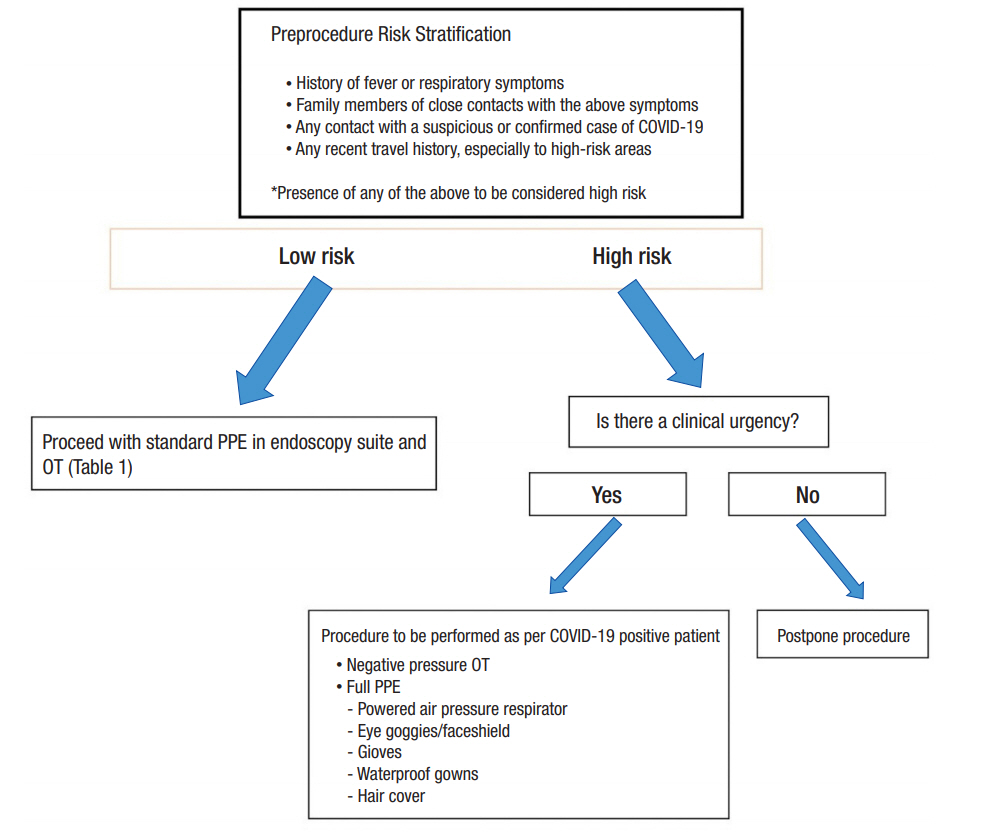
Our workflow for evaluating patients scheduled for procedures (Endoscopy or Surgery) is illustrated in Fig. 1. Preprocedure risk stratification is done for all patients at 3 stages. At the initial anesthetist assessment 1ŌĆō2 weeks preoperatively a chest X-ray or computed tomography thorax for cancer cases will be obtained to assess for consolidative changes in the lungs. Three days prior to the surgery date, our admission team will contact the patient to obtain a travel declaration and to inquire if there are new flu-like symptoms. On day of admission, this process is repeated with a formal declaration form signed by the patient.
Patients who have any travel history within 14 days, or has contact with any member of the public who is positive for COVID-19 or on home quarantine, or has new onset of flu-like symptoms will be advised on postponement of procedure. The procedure would be postponed by 2 to 4 weeks to allow infected patients who may be within the incubation period of COIVD-19 to declare themselves.
If there is clinical urgency, the procedure may proceed with precautions taken as per a presumed COVID-19 positive patient (Fig. 1). Clinical urgency refers to cases which necessitate intervention within 2 weeks. These include colorectal cancer cases with impending obstruction or with overt bleeding resulting in significant transfusion requirements. Postoperatively, such patients will undergo COVID-19 testing and will be nursed in isolation until their test results clear them from COVID-19 infection.
At the current moment, universal COVID-19 testing for all patients undergoing surgery is not performed. We only perform testing for patients who meet the suspect case definition stipulated by the Ministry of Health, Singapore. As of 16 April 2020, the case definition is as follows:
(1) A person with clinical signs and symptoms suggestive of Community-Acquired Pneumonia or community-acquired severe respiratory infection with breathlessness.
(2) A person with an acute respiratory illness of any degree of severity (e.g., symptoms of cough, sore throat, runny nose, anosmia), with or without fever, who, within 14 days before onset of illness had: (a) Travelled abroad (outside Singapore); (b) Close contact with a case of COVID-19 infection.
PROCEDURAL CONSIDERATIONS
Endoscopy
Endoscopy carries an increased risk of COVID-19 infection from droplets inhalation, conjunctival contact and fomite contamination. Upper gastrointestinal (GI) endoscopy is recognized to be a high risk aerosol-generating procedure (AGP) [10]. However, it is important to highlight that colonoscopy may also pose significant risks. The 2019-nCoV has been consistently isolated in stool samples and fecal oral transmission is recognized [11-13]. It remains unknown if gas insufflation during colonoscopy may be considered an AGP. In our unit, we adopt the same PPE measures for colonoscopy as for a gastroduodenoscopy. A summary of our PPE recommendations for endoscopy is summarized in Table 1.
Colorectal surgery
Minimally invasive surgery
There is scant evidence regarding the risks of virus transmission of minimally invasive surgery (MIS) or open surgery. However, data does indicate that laparoscopy can lead to aerosolization of blood borne viruses, although it remains unknown if this applies to COVID-19 [14, 15].
As such, while we still perform MIS procedures, surgeons are recommended to adopt the necessary PPE precautions. (Table 1) Filtration systems applied to trocars for smoke evacuation and safe evacuation of pneumoperitoneum may be considered but the efficacy of such measures remains unknown.
The risks of transanal MIS procedures (taTME - transanal total mesorectal excision, TAMIS-transanal minimally invasive surgery) remains unknown in the COVID-19 era. However, the 2019-nCoV has been demonstrated in stool samples, and with the strong potential risks while evacuating air per-anally, these procedures should be performed with extreme caution in the current climate [11-13,16].
Open surgery
Smoke from electrocautery during open surgery can harbor virus particles [17]. Unlike MIS, the exposure of the surgeon to smoke inhalation is likely higher in open surgery which raises the possibility of COVID-19 transmission. Measures to mitigate risks of transmission should thus be adopted. These, together with our proposed PPE for open surgery, are summarized in Table 1.
Operating room management during surgery
Most operating room (ORs) have an average of 15ŌĆō40 air exchanges per hour. To ensure clean air in the OR, 14ŌĆō18 minutes is thus required [18]. In our institution, an intubation-extubation protocol has been in practice since the COVID-19 outbreak. In this protocol, a 5-minute pause has been mandated during intubation and extubation, with only the anesthetists and assistant in OR wearing full PPE. This ensures at least 2 gas exchanges of the OR, and enhances safety in the scenario that surgeons are operating on an undiagnosed COVID-19 case. To address the concerns of laparoscopy, an additional 15 minutes has been factored in, which commences on evacuation of the pneumoperitoneum. This allows a complete 20 minutes of air exchange on completion of surgery and extubation [19].
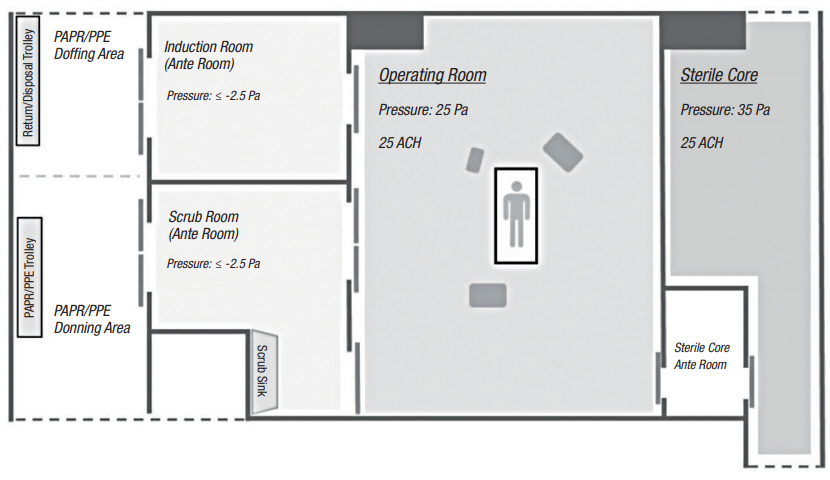
For COVID-19 cases, surgery is performed in a dedicated negative pressure OR. In the negative pressure OR, the induction and scrub room is maintained at a pressure of -2.5 Pascals relative to the exterior to prevent dissemination of aerosolized virus particles. Fig. 2 illustrates the setup of our negative pressure OR.
The COVID-19 pandemic is likely to run a protracted course and has immense implications on colorectal practice. Various academic societies have provided guidance for clinical practice and these are summarized in Table 2 [10, 20-23]. While the measures we have in place have allowed safe colorectal surgery, there are several modifications that may have to be considered in view of increasing community transmission and recognition of presymptomatic transmission. One suggestion is that routine bowel preparation may be considered to reduce fecal load during bowel surgery. Secondly, the appropriate PPE in this era needs to be reviewed and perhaps all OR staff should be in N95 respirators for all colorectal procedures until there is more evidence regarding transmission risk during surgery. The difficulty, however, is having the availability of resources and its pragmatic allocation. Thirdly, universal preoperative COVID-19 testing may seem to be intuitively better and replace clinical stratification but the issues of false negatives and limited COVID-19 testing capacity may hamper widespread implementation. We urge the colorectal fraternity to share their workflows and protocols to ensure safe practice among our community amidst this uncertain era.