INTRODUCTION
A submucosal tumor of the digestive system is defined as a disease that has main lesions located at a layer lower than the mucosa and that is covered with a mucosa identical to the nearby mucosa. It is known to originate from an intramural or an external tumor. The morbidity is known to be approximately 2 to 6% in gastric submucosal tumors, and although it is known to be very low in rectal submucosal tumors, the exact rate has not been reported yet. As identifying the cause or the origin of a submucosal tumor with endoscopic findings alone is very difficult, additional examinations such as endoscopic ultrasonography, a gastrointestinal series, computed tomography (CT) and magnetic resonance imaging (MRI) are required in most cases. A rectal submucosal tumor may be completely treated if diagnosis and treatment are appropriately performed. Thus, early diagnosis is required.
Rectal submucosal tumors can be mainly classified as intramural or external tumors. Intramural tumors include leiomyomas, cysts, lipomas, carcinoid tumors, lymphomas, hemangiomas, and gastrointestinal stromal tumors. Meanwhile, external tumors include direct/indirect metastases of tumors derived from other organs and peritoneal metastatic tumors. Rectal submucosal tumors have various symptoms from no symptoms to abdominal pain, bleeding, intestinal obstruction and overlap, and constipation. In rare cases, a tumor originating from the prostate gland or from an intrapelvic organ such as the uterus or the ovary may cause defecation disorder, such as constipation, due to external invasion or compression of the intestinal tract. However, no case of a primary ovarian lymphoma presenting with defecation disorder as a first symptom has been reported [1, 2]. Accordingly, the authors conducted colonoscopy on a 42-year-old female patient who visited the authors' hospital due to defecation disorder. As a result, a case of primary non-Hodgkin's lymphoma presenting as a rectal submucosal tumor was diagnosed. Thus, the authors report the case with a reference review.
CASE REPORT
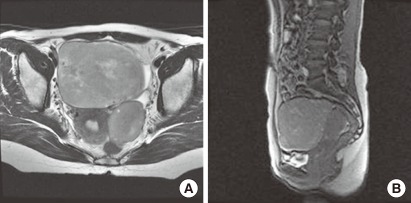
A 42-year-old female patient visited Chungnam National University Hospital due to defecation disorder and lower abdominal discomfort that had been persistent for 6 months. She had had a weight loss of 5 kg over those six months, but had no symptoms such as nausea and vomiting. The patient had no previous history of diseases and particular familial history. Her vital signs were blood pressure, 120/70 mmHg; heart rate, 70 beats/min; respiration rate, 19 beats/min; and body temperature, 36.7℃, and she had clear consciousness. A peripheral blood test showed white blood cell, 4,640/mm3 (neutrophils, 55.3%; lymphatic cells, 32.8%; mononuclear cells, 9.7%; eosinophils, 1.1%); hemoglobin, 12.9 g/dL; and platelets, 281,000/mm3. Serum biochemistry showed blood urea nitrogen, 7.4 mg/dL; creatinine, 0.7 mg/dL; aspartate aminotransferase, 29 IU/L; alanine aminotransferase, 11 IU/L; total bilirubin, 0.6 mg/dL; alkaline phosphatase, 65 IU/L; total protein, 8.2 g/dL; albumin, 5.2 g/dL; and lactate dehydrogenase, 305 IU/L. Tumor marker examination showed carcinoembryonic antigen, 3 ng/mL; carbohydrate antigen 19-9, 2.35 U/mL; and cancer antigen 125, 54.2 U/mL. The result of digital rectal examination conducted to assess the cause of the defecation disorder was normal. On colonoscopy, a giant hemispherical submucosal mass that covered more than 3/4 of the total intralumen and that was covered with a mucosa identical to the nearby mucosa with a smooth surface was found in the rectum. The mass was felt when the mass was pressed using forceps. No sign of rolling was shown, and the cushion sign was shown to be positive. In addition, the intralumen was not spread despite air injection (Fig. 1). To accurately assess the submucosal mass and lower abdominal discomfort that had been present during menstruation and had been severe for six months, we conducted abdominal and vaginal ultrasonography. As a result, a mass was observed in the bilateral ovary (Fig. 2). Thus, MRI was immediately conducted without endoscopic ultrasonography. In MRI, a 9.2 × 9.3 cm mass with unclear contrast enhancement was observed in the right ovary, and a 5.4 × 5.3 cm mass was observed in the left ovary (Fig. 3). The right ureter was obstructed by the tumor, and the proximal ureter was slightly extended. No additional intraabdominal lymphadenopathy was observed.
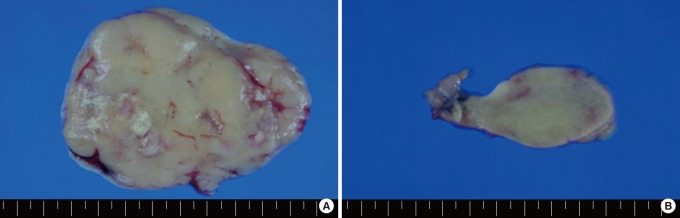
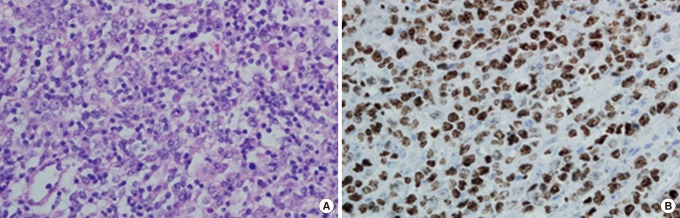
Based on the aforementioned findings, the patient was diagnosed with a malignant tumor originating from the bilateral ovary. Subsequently, a laparotomy with an incision along the lower abdominal midline was conducted under systemic anesthesia. No other metastatic lesion was observed in the abdominal cavity. The patient underwent a bilateral oophorectomy and hysterectomy. In the gross findings, the sizes of the right and the left ovaries were 11 × 9 × 5 cm and 7 × 5 × 5.3 cm, respectively (Fig. 4). The surface of the endothelial membrane was smooth, and a solid mass with a homogenous dissectional plane was observed. In addition, partially necrotized tissues were found, and the mass was shown to have compressed the rectum, but not to have directly invaded the rectum. On microscopic examination, the tumor cells consisted of diffuse large lymphocytes, had abundant cytoplasm, and were eosinophilic. They had blistered nucleus and nucleoplasm that was agglomerated along the nuclear membrane. Two to four nucleoli were found to be close to the nuclear membrane, or one nucleolus was found in the center of the nucleus. The tumor cells were positive to CD20, a marker of B lymphocytes. The Ki-67 labeling index was 80%, which was high.
Based on the aforementioned findings, the patent was diagnosed with a diffuse large B-cell lymphoma (Fig. 5). After the surgery, positron emission tomography (PET)-CT and abdominal CT were conducted, and the results showed no residual lesion. An examination of bone marrow tissue showed no evidence of bone marrow invasion. The patient recovered without particular complications after the surgery and has completed the 6th cycle of anticancer therapy using the CHOP (cyclophosphamide, hydroxydaunorubicin, vincristine, prednisolone) regimen. Defecation disorder and lower abdominal discomfort were also improved, and the patient showed good performance status.
DISCUSSION
A malignant lymphoma is a malignant tumor that is derived from reticuloendothelial cells or lymphatic cells present in lymph nodes and lymphatic tissues. It mainly occurs in lymph nodes, but also occurs in other tissues in rare cases. The incidence rate of malignant lymphomas has been reported to be 10 to 58%. A primary lymphoma mainly invades the gastrointestinal and the upper respiratory systems. The incidence rate of lymphomas in locations other than the primary lymph node of the pelvis, such as the retroperitoneal space, the ovary, the uterine corpus, the uterine cervix, and the vagina is known to be very low. In particular, primary malignant lymphomas that occur in the ovaries account for 1.5% of ovarian tumors and 0.5% of all cases of non-Hodgkin's lymphoma, which is a very rare disease [3].
The mean age of the onset of ovarian lymphoma is 33 years, but the mean age of the onset of primary ovarian lymphoma is 41.8 years. Primary ovarian lymphoma occurs more frequently in elderly patients than secondary ovarian lymphoma, has pelvic or abdominal pain as its main symptoms, and is known to be accidentally found in approximately 1/3 of patients during surgery due to its being asymptomatic. In addition, as shown in this case, patients complain of defecation disorders such as constipation in rare cases. Defecation disorder commonly occurs due to mechanical obstruction of the rectum. If the rectal angle at which the puborectalis muscle is located is compressed, symptoms such as constipation, tenesmus, fecal thinning, and fecal incontinence may occur. A bilateral internal iliac artery aneurysm, benign prostate hyperplasia, and giant bladder diverticulum are known to be rare causative factors for mechanical obstruction of the rectum due to external compression of the rectum [4-6]. A domestic study reported that gastric cancer accounted for 31 (79.5%) out of 39 malignant tumors, except for rectal cancer in which case the patients underwent rectal stent insertion as a conservative management due to colon obstruction, and that ovarian cancer accounted for one case (2.6%) [7].
In another study, endoscopic ultrasonography was conducted on 40 patients with colorectal submucosal tumors. Rectal carcinoid tumors accounted for 13 cases, which was the most common disease, and five cases of rectal stromal tumors with muscular origin, 2 cases of compression by uterine myomas, and one case of cecal cancer were also reported [8]. When the authors reviewed relevant literature, no case of primary ovarian lymphoma presenting as a submucosal tumor was found [1, 2]. In the case reported here, the patient who complained of defecation disorder and lower abdominal discomfort and who subsequently underwent colonoscopy was diagnosed with a submucosal tumor and showed partial rectal obstruction due to external compression. Subsequently, on a histologic examination conducted after the surgical removal of the mass, the patient was diagnosed with primary ovarian lymphoma.
In primary ovarian lymphoma, abdominal pain, abdominal mass palpitation, and ascites are the most common symptoms that first appear. Thus, no difference in symptoms is found between primary ovarian lymphoma and ovarian cancer [9, 10]. Symptoms such as fever, night sweats, and weight loss are reported in 10 to 33% of patients [3, 9]. No case of primary ovarian lymphoma diagnosed based on a complaint of defecation disorder due to rectal compression from outside the rectum has been reported so far [2]. Bilateral primary ovarian lymphoma is rare, and although its size is very small, sometimes it can be very large. In a histological perspective, a diffuse large B-cell lymphoma is known to be the most common type, and tumors to be screened include granulosa-theca cell tumors, dysgerminomas, small-cell carcinomas, and granulocytic sarcomas [10-12]. CT is useful in the determination of disease stage, and bone marrow aspiration is also required. PET-CT is useful in the determination of disease stage, as well as in the assessment of postoperative response. Until now, 11 cases of primary ovarian lymphoma have been reported in Korea [1]. As primary ovarian lymphoma is rare, its treatment method has not been completely established yet. Thus, in most cases, as in the case of the patient of this case report, combination chemotherapy, such as the CHOP regimen, after a hysterectomy and surgical removal via an adnexectomy is conducted. However, in the case of primary ovarian lymphoma locally restricted to the ovary, the long-term survival rate after combination chemotherapy is 75%, a pretty good prognosis [3]. No difference in failure-free survival is found between primary ovarian lymphoma and lymphoma from the lymphatic system [13].
Many studies reported that primary ovarian lymphoma had a mean survival period of less than 3 years [3]. Zhao et al. [2] reported that for 13 cases of diffuse large B-cell lymphoma among primary ovarian lymphoma, the median overall survival was 24 months and that poor prognostic factors were age, Karnofsky performance status, and ascites.
In summary, primary ovarian lymphoma is a very rare disease. Most patients visit the hospital due to abdominal pain, pelvic pain, or abdominal mass palpation. The authors experienced a case of primary ovarian lymphoma presenting as a rectal submucosal tumor, which is rarely reported among causative factors that may cause defecation disorder by rectal compression. Accordingly, the authors report the case with a reference review.