INTRODUCTION
Matrix metalloproteinases (MMPs) are enzymes that degrade extracellular matrices. These enzymes mediate not only normal physiological functions, such as tissue remodeling and development of organs, they also play a role in pathologic condition, such as regulation of inflammatory reactions, tumor growth and metastasis [1]. The roles of MMP in cancer growth and metastasis are related to their degradation of extracellular matrices, pertinent to cell adhesion and migration, and secretion of growth factors, cytokines, vascular growth factors. Studies on MMP have been conducted in breast cancer, pancreatic cancer, lung cancer, colorectal cancer, ovarian cancer, prostate cancer, and brain cancer, and based on those studies, cancer treatment that apply MMP suppressors have been attempted [2].
According to the 2008 Korean survey, colorectal cancer is the 4th leading cause of death (9.9%) among all cancers, and recently, it has shown an increasing trend in Korea [3]. The prognosis for colorectal cancer is relatively good. Nonetheless, the 5-year survival rate of TNM stage III cancer with lymph node metastasis is merely 25-60%. In this stage, postoperative adjuvant chemotherapy has been reported to improve the prognoses for patients; however, many patients die due to recurrence and metastasis of the cancer. In stage II cancer without lymph node metastasis, the effect of chemotherapy is not clear yet [4]. In colorectal cancer, the most important prognostic factor is, of course, the stage of tumor. Nevertheless, it is important to find new prognostic factors as a basis for determining the prognoses for patients, follow-ups, and post-surgical treatments. MMPs have been investigated in regard to tumor growth and metastasis, and in colorectal cancer, they have been reported to play an important role in the development and growth of tumors and in the metastasis process [5]. However, the results of studies that examined whether MMPs were significant prognostic factors in colorectal cancer are contradictory in many cases [2]. The authors examined the expressions of MMP-2 and MMP-7 in colorectal cancer, and their significance as prognostic factors was examined by investigating the expression characteristics, the association with other pathological findings, and the association with the prognoses for patients.
METHODS
Subjects
The study was conducted on 144 patients who were diagnosed as having as colorectal adenocarcinoma and who underwent a resection from January 1998 to August 2004.
Clinicopathological factors
Based on clinical records and pathology reports, the location of the tumor, serum CEA, T-stage, lymph node metastasis, distant metastasis, pathological differentiation grade, lymphatic invasion, macroscopic morphology of tumor, and recurrence were examined. Based on the splenic flexure, the area of the colon was classified based as the right colon or the left colon. The upper border of the rectum was defined as being 15 cm away from the anal verge. For the prognoses for patients, we analyzed the overall survival rate and the disease-free survival rate. Follow-up observations were performed until December 2009, and the average follow-up observation period was 61.8 months (range, 2 to 133 months). Survivals were assessed based on clinical records and telephone interviews.
Immunohistochemical staining methods
Tissue arrays were prepared by consigning them to the SuperBioChips, Co. (Seoul, Korea). Tissue array blocks were sectioned with 4-┬Ąm thicknesses, and immunohistochemical staining was performed. Paraffin was removed, and to suppress endogenous peroxidase, the samples were treated with 0.3% hydrogen peroxide. The samples were reacted with primary anti-MMP-2 antibody (clone A-Gel VC2, 1:400 dilution; Neomarkers, Fremont, CA, USA) or primary anti-MMP-7 antibody (clone ID-2, 1:1,500 dilution; Chemicon, Temecula, CA, USA) at room temperature for 1 hour, washed with phosphate-buffered saline, reacted with biotynylated secondary antibody, and incubated with avidin-biotin streptavidin-peroxidase complex (Vectastatin Elite ABC kit; Vector Laboratories, Burlingame, CA, USA). As dyes, 3,3'-diaminobenzidine tetrahydrochloride was used, and counter staining was done with Mayer's hemotoxylin. The negative control group was stained by using the identical procedure, but omitting the first antibody. Immunohistochemical staining of the specimens was evaluated by one pathologist (a co-author). The criterion for a positive expression was more than 10% of the cytoplasm showing a distinct expression higher than moderate levels. In regard to MMP-2, the expressions in the central and the border areas of the tumors and in the interstitium around stumor cells were examined. In regard to MMP-7, only the expressions in the centers of tumor cells and in the border areas of the tumors were examined. MMP-2 has been reported to be primarily produced by interstitial tissues and MMP-7 to be primarily produced and expressed by epithelial cells [6]. In the preliminary experiments of our study, no expression of MMP-7 in the interstitium was observed; thus, the expression of MMP-7 in the interstitium was not examined.
RESULTS
Expressions of MMP-2 and MMP -7 and their correlation
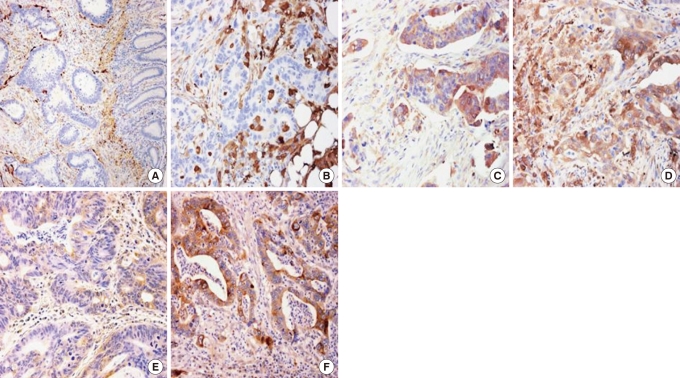
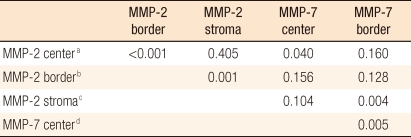
MMP-2 was expressed in the central area of the tumor in 24 cases (16.7%), in the border area in 56 cases (38.9%), and in the interstitium in 40 cases (27.8%). MMP-7 was expressed in the central area of the tumor in 10 cases (6.9%) and in the border area in 34 cases (23.6%) (Fig. 1, Table 1). The expression of MMP-2 in the central area correlated significantly to the expression MMP-2 in the border area (P < 0.001) and to the expression of MMP-7 in the central area (P = 0.04). The expression of MMP-2 in the border area correlated significantly to the expression of MMP-2 in interstitial tissues (P = 0.001), the expression of MMP-2 in interstitial tissues significantly correlated to the expression of MMP-7 in the border area (P = 0.004), and the expression of MMP-7 in the central area correlated significantly to the expression of MMP-7 in the border area (P = 0.005) (Table 2).
Comparison of the expressions of MMP with clinicopathological factors
When expressions of MMP were compared with clinicopathological factors, positive expressions of MMP-2 in the border areas in the right colon, the left colon, and the rectum were observed in 8 out of 34 patients (23.5%), in 18 out of 44 patients (40.9%), and in 30 out of 66 patients (45.5%), respectively. A trend was noted in that MMP-2 was expressed more toward the distal bowel (P = 0.098). The expression according to T stage was 11.1% in T1 (1/9), 33.3% in T2 (5/15), 46.2% in T3 (49/106), and 7.1% in T4 (1/14) (P = 0.001). Concerning the expression of MMP-2 in interstitial tissues, the positive rate for the right colon was 8.8% (3/34), that for the left colon was 29.5% (13/44), and that for the rectum was 36.4% (24/66). Expression was clearly higher toward the distal bowel (P = 0.014). MMP-7 was expressed in the border area of the tumor in 21 out of 109 fungating tumor cases (19.3%), and in infiltrative cases, it was expressed in 13 out of 35 cases (37.1%) (P = 0.04). Tumor markers, lymph node metastasis, distant metastasis, tumor differentiation grade, lymphatic duct invasion, and recurrence were examined. Nevertheless, factors that correlated to the expression of MMP were not found (Table 3). The association of the expression of MMP-2 or MMP-7 in the central area of the tumor with clinicopathological factors was also examined, but no statistically significance differences were found.
Expressions of MMP-2 and MMP-7 and the prognosis for the patient
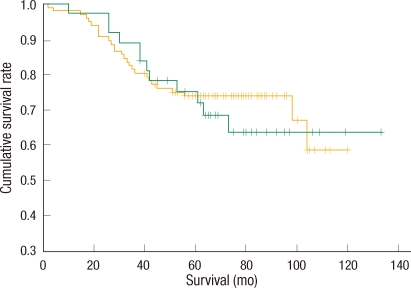
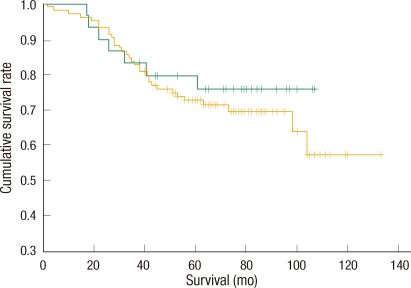
Among 144 patients, in the 136 patients who underwent curative resection, the overall survival rate and the disease-free survival rate according to the expressions of MMP-2 and MMP-7 were examined. The 5-year survival rate of the patients with positive expression of MMP-2 in the border area was 75.3%, and that of patients with negative expression was 73.6% (P = 0.7955) (Fig. 2). The 5-year survival rate of patients with positive MMP-2 expression in interstitial tissues was 75.2%, and that of patients with negative expression was 74.0% (P = 0.7340) (Fig. 3). The 5-year survival rate of patients with positive MMP-7 expression in the border area was 79.9%, and that of patients with negative expression was 72.8% (P = 0.5175) (Fig. 4). The 5-year disease free survival rates of patients with positive and negative expressions of MMP-2 in the border area were 68.4% and 70.3% (P = 0.8290), respectively. The 5-year disease-free survival rates for patients with positive and negative expressions of MMP-2 in interstitial tissues were 65.3% and 71.1% (P = 0.8171), respectively. The 5-year disease-free survival rates of patients with positive and negative expressions of MMP-7 in the border area were 66.1% and 70.5%, respectively, but this difference was not statistically significant (P = 0.7682). The association of the expressions of MMP-2 or MMP-7 in the central area of the tumor with prognosis was examined, but no significant result was found.
DISCUSSION
MMPs are kinds of enzymes that degrade extracellular matrices, and they act under both normal physiologic and pathologic conditions. Twenty-four types of MMPs, including 5 types of secreted MMPs and 3 types of membrane bound MT-MMPs, have been reported. In regard to tumors, most MMPS are produced and secreted by interstitial tissues in the vicinity of the tumor in response to the stimulation of tumor cells [7]. Until recently, MMPs have been reported to exert effects on the process of tumor invasion and metastasis. Recently, they have also been reported to play an important role in the early development of tumors [8].
In regard to the early oncogenic process of colorectal cancer, primarily MMP-7 has been investigated. In a study that examined the expression of MMP-7 in dysplasia that developed in ulcerative colitis, in low-grade dysplasia, it was shown to be expressed less, and in high-grade dysplasia and cancer, the expression of MMP-7 was clearly shown, thus establishing that MMP-7 played a role in the early phase of cancer development [9]. In addition, in a study conducted on liver metastasis of colorectal cancer, Zeng et al. [10] examined the expression of MMP-7 and observed that MMP-7 mRNA and enzyme activity were over-expressed in metastatic cancer tissues in comparison with normal liver tissues, and in immunohistochemical staining, the border area of the cancer showed strong expression of MMP-7; thus, MMP-7 played an important role in liver metastasis of colorectal cancer.
Some investigations of the association of MMP-2 expression with distant metastasis of colorectal cancer have been performed. Brand et al. [11] reported a significant reduction of liver metastasis in animal experiments using the gene of the MMP-2 suppressor, the tissue inhibitor of MMP-2 (TIMP-2). In patients with the elevated levels of plasma MMP-2, lymph node metastasis has been reported to occur more frequently [12].
In our study, the expression of MMP-2 in tumor tissues and interstitial tissues, as well as the expression of MMP-7 in tumor tissues, were examined by immunohistochemical staining. Others have reported that MMP-7 is produced by epithelial cells and that it is not expressed in the interstitium [6, 13]. In our preliminary experiments, MMP-7 was not expressed in the interstitium. MMP-2 was expressed in the central areas of the tumors in 16.7% of the cases, and in the border areas in 38.8% of the cases. MMP-7 was expressed in the central areas of tumors in 6.9% of the cases, and in the border areas in 23.6% of the cases. This is in agreement with the results of most studies that examined the expressions of MMP-2 and MMP-7 by immunohistochemical staining; i.e., MMP was strongly expressed in the borders of the tumors, in other ward, in cancer cells in the front lines of cancers that invade normal tissues [10, 13-16].
Previous studies have reported that MMP-2 is produced primarily by fibroblasts in interstitial tissues and is activated in tumor cells [17] and that during the process, the mutual action of tumor cells and interstitial cells is important [18]; this can be explained by MMP-2 being expressed strongly in the border areas of tumors where tumor and interstitial tissues are abundant. MMP-7 was also observed to be expressed strongly in the border areas of tumors, and similar to MMP-2, this was explained by some investigators as being due to the mutual interaction of tumors and host cells [16]. Such strong expression of MMP in the border area is thought to accelerate the degradation of the tumor matrix and to activate tumor invasion and metastasis.
No studies have reported expressions in the central area and the border area separately as our study has done. Most studies examined and reported the expression of MMP in the border area, and MMP-2 was expressed in 35-87% of the cases [13-15], and MMP-7 was expressed in 54-84% of the cases [13, 14, 19]. In our study, the expression rate was low, but the standards for evaluation were different; thus, objective comparisons are difficult. In our study, the expression of MMP-2 in the border areas of tumors and in the interstitium were 38.9% and 27.8% (P = 0.001). This may be explained sufficiently by the mutual relation of tumor cells and interstitial tissues that was described above. In regard to the site of the expression of MMP-2, Schwandner et al. [13] reported that it was expressed in tumor cells in 35% of the cases and in the interstitium in 77% of the cases. Hilska et al. [14] reported that MMP-2 expressions in tumor cells and in the interstitium were comparable in 87% of the cases. Papadopoulou et al. [20] reported that MMP-2 was expressed in tumor cells in 44% of the cases and in the interstitium in approximately 50% of the cases. Nonetheless, the staining intensity of the interstitium was weaker than that of tumor cells. Such differences appear to be due to differences in research and assessment methods.
In our study, in the central areas of tumors, the expressions of MMP-2 and MMP-7 correlated (P = 0.04), and in the interstitium, the expression of MMP-2 was associated with the expression of MMP-7 in tumors in the vicinity (P = 0.004). This is a result that is in agreement with research reports showing that MMP-7 contributes to the activation of pro-MMP-2 [21].
When the expression of MMP is compared with clinicopathological factors, MMP-7 was expressed in the border areas of macroscopic elevated type tumors in 19.3% of the cases, in invasive type tumors with unclear borders, it was expressed in 37.1% of the cases (P = 0.03), and in areas where tumor invasion was active, it was found to be expressed well. However, it was not associated with disease stage, tumor differentiation grade, tumor markers, lymphatic duct invasion, distant metastasis, and recurrence. In regard to the expression of MMP-2 in the interstitium, it was expressed in the right colon in 8.8% of the cases, in the left colon in 29.5% of the cases, in the rectum in 36.4% of the cases; toward the distal bowel, it was expressed more (P = 0.014). In the colon, the expression of MMP-2 in interstitial tissues was 20.5%, and in the rectum, it was 36.4%, and that difference was significant (P = 0.034). This is different from the results of other studies in which the expressions of MMP-2 in the colon and the rectum were not different [22, 23]. Nevertheless, because of the different study methods, the results are difficult to compare. However, MMP-2 is produced mainly in the interstitium [24]; thus more significant results may be obtained by assessing the expression in the interstitium. The expression of MMP-2 did not correlate to the prognostic factors of colorectal cancer patients, such as tumor stage, tumor cell differentiation grade, tumor markers, lymphatic duct invasion, distant metastasis, and recurrence.
In our study, the prognoses of patients based on the expressions of MMP-2 and MMP-7 were not different. Concerning this point, many studies have reported contradictory results. Cho et al. [25] reported that MMP-2 was not associated with several clinicopathological factors that show tumor invasiveness. Schwandner et al. [13] also reported that in rectal cancer, MMP-2 and MMP-7 expressions were not associated with prognosis. On the other hand, Hilska et al. [14] reported that the prognosis of colon cancer patients with the expression of MMP-2 was poor. Sundov et al. [15] reported that in disease stage Duke's B colon cancer patients, the expression of MMP-2 was a poor prognostic factor. Adachi et al. [16] reported that the expression of MMP-7 was an independent prognostic factor in patients with colorectal cancer. By measuring the serum MMP-7 of patients, Maurel et al. [26] observed that it was elevated in cases of advanced colorectal cancer, and that it was an independent prognostic factor. Because of such varying reports, it appears to be difficult to answer definitely the question of whether a specific MMP is a significant prognostic factor. As neovascularization of a tumor is achieved by the coordination of its stimulating factors and antagonistic factors, the action of MMP, which is associated with tumor invasion and metastasis, must be understood within its relationship with the inhibitory factors that areTIMP [27].
In colorectal cancer, MMP-2 and MMP-7 were expressed more strongly in the border areas of tumors than in the central areas. In our study, the expressions of MMP-2 or MMP-7 did not significantly correlate to an advanced level of cancer; similarly, it had no correlation with the prognoses for patients.